Sensorimotor therapy: Physical and psychological regressions contribute to an improved kinesthetic and vestibular capacity in children and adolescents with motor difficulties and concentration problems
Main Article Content
Our aim was to gain increased understanding of the effects of sensorimotor therapy on the physical and psychological development of children and young people when using the method Retraining for Balance. The records of 8 children who had completed the program were randomly selected from a cohort of 232 with sensorimotor difficulties and concentration problems. The participants, 7 boys and 1 girl, averaged 9 years of age. The Empirical Phenomenological Psychological method (the EPP-method, Gunmar Karlsson, 1995) was used for this analysis, which resulted in 29 categories which yielded 3 overarching themes: a) the introduction of sensorimotor exercises, b) regression to earlier sensorimotor and psychological behaviors, and c) transformations in which the sensorimotor and psychological skills of the children matured and developed. The themes formed the kinesthetic-vestibular developmental model illustrating how sensorimotor exercises push the therapy process forward while recurrent regressions are followed by positive developmental phases. The results of the study were generalized to the remaining 224 children in the cohort by comparing each individual’s records to the kinesthetic-vestibular model.
Sensorimotor training can be conducted for different purposes and in several different ways (McPhillips, Hepper, & Mulhem, 2000; Pless, 2001). The purpose of therapy according to the method Retraining for Balance (Niklasson, Niklasson, & Bergström, 1999, 2007) is primarily to enhance the physical maturity and sensorimotor development of children and adolescents, through stereotypic infant movements consisting of vestibular and kinesthetic stimulation. In line with the opinions of researchers including Adolph, Bertenthal, Boker, Goldfield, and Gibson (1997), Capute and Accardo (1991), and Goldfield (1989) the method stresses the importance of the client passing through the gross motor milestones of creeping and crawling. Clients are predominantly clumsy children with concentration problems who underachieve at school. An essential element of the method is the fact that the parents carry out the therapy in the secure context of home (Niklasson, Niklasson, & Norlander, 2009). This notion is in line with Schilder (1964, 1971) and Erikson (1987), who argue that there is an association between the development of movement and the development of emotions. Both of them emphasize the important role of the parents in this process. During therapy clients have exhibited different kinds of regressive behaviors including psychological regressions such as increased childlike behaviors and physical regression such as temporary setbacks in motor functions. Goddard (2002) also noted various types of regressions in the context of similar training, and Downing (1997) used the concept of “bodily regression” referring to an experience of an early memory from childhood while working with somatic therapy. The concepts of maturation and development (Holt, 1991) are sometimes used synonymously although maturation is a process of ripening while development is a process of unfolding. When it comes to sensorimotor development, different skills occur in an orderly sequence but the age of emergence (maturation) varies among children (Capute & Accardo, 1991; Passer & Smith, 2001). The faculty of movement of the newborn is highly stereotypic (Guyton, 1991; Thelen & Fisher, 1983) and is dominated by involuntary movements of the reflexes. Primary (or primitive; McPhillips et al., 2000) reflexes are a set of about 70 (Illingworth, 1987) brainstem mediated behavioral movement patterns which emerge during fetal life, some of which are closely connected to the vestibular system. During the first year of life, as the child adapts to gravity, the nervous system matures to be able to perform more voluntary movements. Vestibular stimulation activates the muscle tone, inhibits primary reflexes, and promotes postural responses (Morrison, 1985; Paine et al., 1964; Robbins, 1977). The primary reflexes are inhibited and postural responses (body righting reactions) and gross motor milestones such as rolling, creeping (locomotion in prone), and crawling (locomotion in quadruped) develop (Capute & Accardo, 1991; Morrison, 1985). The development of gross motor milestones coincides with the period, 6-12 months, when the vestibular system is most receptive to stimulation (Ornitz, 1983). It is most likely that during the period when the child is creeping and crawling, a more mature sense of balance develops (Maurer & Maurer, 1989). According to Bee (1992) the child’s experiences are affected by its physical ability and physical changes trigger new behaviors. Using the concept Psychological development Levin (1991) suggested that the brain, when responding to experience using its property of plasticity, can change its organization in the process of learning. This unfolding process follows the evolution of learning-related subsystems in the brain and is the result of specific changes in brain organization which together will form a unique brain with special learning capabilities. The process starts with the cerebellum which is metabolically very active from the first day of life and therefore a contributor to early motor memories involving sensory modalities. Cuddling or rocking an infant (Restak, 1980) sends impulses directly to the cerebellum which stimulate its development. Consistent with the findings of Stern (1985) the concept of core- self would be based on these early cerebellar (sensorimotor) memories. Eventually the cerebellar memory system becomes the vestibulocerebellar system (VCS) and Levin speculates that its connection with the cortex is of importance when it comes to the establishment of an early physical self-cohesiveness. Besides the VCS-cortical system there is a vestibulo-thalamocortical pathway (Brodal, 1981; Purves et al., 1997). According to Prescott (Restak, 1980) the cerebellum might be involved in complex emotional behavior as a regulator for motor and sensoriemotional processes.
Rothschild (2000) argued that all memories have a sensory basis and that the memory of an earlier experience may be elicited if it is stimulated by a similar sensory event. She also distinguished between exteroceptive (external) and interoceptive (internal) sensory systems. Interoception primarily takes place through proprioception (conscious and subconscious patterns of movement), of which the kinesthetic and the vestibular senses are a part. The kinesthetic sense is active during learning and during the encoding of memories of movements, and it is also connected to procedural memory (i.e., how a movement is acquired), whereas the memory function of the vestibular system (Berthoz, 2000) is connected to rotational and to linear, passive movements. The importance of movement was also emphasized by Thelen and Smith (1994), who argued that movement per se should be considered a perceptual system. Levine and Frederick (1997) used the concept of a “felt sense”, (i.e., internal, bodily sensations) in traumatized clients. The sensations constitute a gateway through which the trauma may be accessed more softly, a notion in line with Berthoz’ argument concerning a type of neuro-ethology which illustrates the association between natural movements and the feelings elicited by the movements.
The concept of psychological regression has been dealt with in different ways in the literature. Freud (1980) described regression as a return to an earlier stage of libidinal development. In psychotherapy, regressions are typically seen as sexuality and neuroses which damage the ego, but there are also regressions serving the ego (Haak, 1982; Kris, 1952), regressions which allow the pleasure principle to dominate facilitating “a new beginning” (Balint, 1968). Under such circumstances the ego itself is in charge. Winnicott (1991) argued that such regressions are of a healing nature capable of improving previous experiences and that the return depends on regaining independence. Barnes and Berke (1991) described regression as a return to childhood and as a way to recover. Regression is, however, not only about healing but it should rather be seen (Battegay, 1970; Berns, 1966) as a necessary step in maturation. Werner (1957) and Loewald (1981) both argued that regression and progression are necessary and complementary with regard to an organization of the psychological level and the same argument is held for physical development (McGraw, 1995). It can also be described as the way in which the brain reorganizes itself in that an older neural circuit is used, while at the same time circuits established later are blocked in order to be modified and reorganized (Bach-y-Rita, 2004; Doidge, 2007). It is likely that the immature brain of the child is more open to regressions due to its instability, given that neural circuits are not yet established (Bergström, 1969).
While working with Retraining for Balance children and adolescents frequently exhibit both physical and psychological phenomena of regression which appear to precede and enhance physical and psychological maturity and development. The purpose in the current study was to describe these phenomena in order to gain a more thorough understanding of how sensorimotor therapy may have an influence on the physical and psychological development of children and youth.
Method
Participants
The study group comprised 8 children and adolescents, seven boys and one girl, who had all completed the Retraining for Balance therapeutic program (see the “Design” section) at the movement school The Vestibularis Institute. The mean age of the children was 8.75 years (SD = 3.77, age range = 5 to 17) at the start, and the training period was 38.88 months on average (SD = 15.73). The participants were from the middle areas of Sweden, and all had been referred by one or both parents. The number of visits to complete the training program was 16.63 on average (SD = 3.66). Four of the children exhibited delayed language development, as reported by their parents, a reliable marker of a need for sensorimotor training (Gaines & Missiuna, 2007; Goddard, Blythe, & Hyland, 1998; Rintala & Linjala, 2003). One child had been diagnosed as having attention-deficit hyperactivity disorder (ADHD).
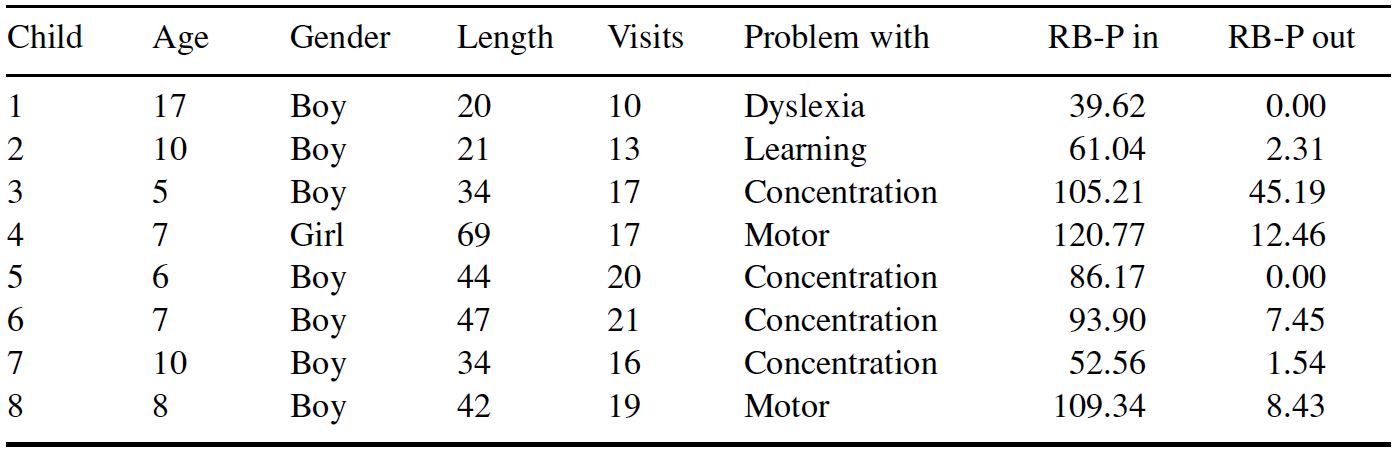
The parents provided the reason for the referral to the training, and four of them reported “concentration problems”, two indicated “motor difficulties, clumsiness”, one “reading difficulties”, and one “learning difficulties”. Following the training program five of the parents reported that the children showed a “marked, positive change”, while three of the parents indicated that the children showed “some positive change”. The children were also given a comprehensive sensorimotor test, Retraining for Balance-Physiological Test (RB-P; Niklasson & Niklasson, 1999, 2007), on which their deviation from appropriate age levels on each subtest was noted on a quantitative, 5-point scale ranging from 0 to 4. Similar 5-point scales were used by McPhillips and Sheehy (2004) and by Goddard Blythe (2005). The test is used to measure the sensorimotor maturity of the participants with regard to primary reflexes, postural reactions, gross motor milestones, and vestibular ability. The subtest was created on the basis of research and documentation of the motor development of normal and developmentally delayed children (Capute & Accardo, 1991; Capute, Shapiro, Palmer, Accardo, & Wachtel, 1981; Fiorentino, 1981; Holt, 1991; Illingworth, 1987) and consists of 41 different tests in the latest version (Niklasson & Niklasson, 2007). Several of the tests were selected from the manual Towards Developmental Re-Education (Field & Blythe, 1989) and others came from other sources or were developed at Vestibularis (Niklasson & Niklasson, 1999, 2007). The average score gained by the eight children on the RB-P – where a lower score is an indication of better performance – was 83.58 (SD = 29.35) at the start of training and 9.67 (SD = 15.04) upon completion. A Wilcoxon Signed Ranks Test indicated that the difference was significant (Z = -2.52, p = 0.012) indicating an enhanced sensorimotor ability. For more specific information on participants see Table 1.
Table 1. Retraining for Balance: Summary
Design
The participants completed the training program Retraining for Balance – Methods (RB-M; Niklasson et al., 1999, 2007). The method consists of seven parts. For more information see section below “Retraining for Balance”. The training was carried out at home under the guidance of the parents. The treatment period was close to three years on average, and the participants did the exercises for about 15 minutes per day. Throughout the training period progress was assessed at visits to The Vestibularis Institute at 8-week intervals. At each visit relevant sensory and motor abilities were assessed and the participants showed how the training was conducted at home. Thereafter a new training program was introduced. Each time the children and their parents reported on the results of the training and meticulous notes were kept. In this way, records were created with personal flow charts describing the experiences of the training of each participant as well as the perception of the training by the parents.
Retraining for Balance
The Retraining for Balance method (Niklasson et al., 1999, 2007) consists of seven parts:
(a) Fetal and infant movements Specific stereotypic movement sequences with the purpose of integrating remaining primary reflexes. An example of such a movement is “The Knot” (Niklasson et al., 1999, 2007; Rood, 1956; Stockmeyer, 1967). Each participant lies on his/her back with the arms stretched out at a 90 degree angle, blindfolded and with his/her head on a thick pillow. The head, arms, and legs are slowly lifted at the same time, after which the chin is brought toward the chest, the arms are crossed over the chest, and the legs are crossed in the air. Then there is a return to the starting position.
(b) Vestibular stimulation Wave-like motions and rotations with the purpose of facilitating the integration of the primary reflexes. An example of such a movement is “The Rotation” (Guyton, 1991; Niklasson et al., 1999, 2007; Vose, 1986). The participant sits on a rotating chair with his/her legs in the tailor’s position, and with his/her arms across the chest. The participant is rotated both clockwise and counterclockwise at different speeds. A blindfold is used during most of the training sessions but is removed toward the end of the training (Arnold, Clark, Sachs, Jakim, & Smithies, 1985).
(c) Auditory, perceptual stimulation Auditory perceptual stimulation constitutes a complement to the vestibular training (Brodal, 2004; Frick & Hacker, 2001; Halmagyi, Curthoys, Colebatch, & Aw, 2005; Kolb & Whishaw, 1990; Storr, 1993; Wilson-Pauwels, Akesson, & Stewart, 1988) for the purpose of strengthening the dominance of the right ear (McFadden, 1993; Okamoto, Stracke, Ross, Kakigi, & Pantev, 2007). The participants listen through headphones to especially composed (custom made) music during rest (Holbech, 1986) for 10 minutes per day for an average of 25 weeks. The music was recorded in such a way that the right ear was stimulated more than the left ear.
(d) Tactile stimulation Exercises with the purpose of first stimulating the deep tactile sense of the skin and then stimulating the surface. An example of how the deep tactile sense of the skin may be stimulated is “The Clip” (Niklasson et al., 1999, 2007). The participant lies on his/her back in his/her bed and the parent squeezes one body part at a time and mentions its name. The surface tactile sense is stimulated through light brushes or through light massage.
(e) Gross motor basic movements/milestones An example of such a movement is rolling (Holle, 1985). The participant lies on his/her back on the floor with his/her arms stretched above. The rolling then takes place through head lifts and a shifting of weight.
(f) Sports-related gross motor exercises Exercises at a functional level, that is, standing in an upright posture. Correctly performed exercises require a motor level of development toward increased mobility of the wrists and ankles and stability of the stretching patterns of the body. An example of such a movement is using a skipping rope.
(g) Complementary play exercises Games with the purpose of either preparing the participant for one of the chief exercises of the method or bridging some of the main movements. An example of such a movement is “Wrestling in prone position” (Niklasson et al., 1999, 2007). The participant and a parent lie across from one another on the floor. They grasp each other’s hands and wrestle.
Procedure
In a previous study (Niklasson et al., 2009), in which a total of 232 children and adolescents received sensorimotor training in accordance with the method Retraining for Balance, positive sensorimotor (physical) and psychological effects were shown. In all cases the parents of the clients allowed The Vestibularis Institute to keep the records and other documents, thereby consenting to future evaluations and publications. In order to gain a more thorough understanding of the effective mechanisms of the treatment, the current qualitative study was conducted by examining a sample of the participants. It was done by randomly selecting eight cases from the 232 children. The empirical data consisted of the records containing the flow charts and the notes from each return visit. Given that the children sometimes found it difficult to verbalize their experiences, the parents’ reports were of significance. In traditional phenomenological methodology the experiences of the clients themselves constitute the basis. In the current study experiences in the third person are thus also included. Dennett (1991, 2003) referred to that procedure as hetero-phenomenology. Gallagher (1997) argued that there is no difference between third person reports and phenomenology in a traditional sense.
Processing the Data
The Empirical Phenomenological Psychological Method (EPP-method) devised by Gunnar Karlsson (1995) was used in processing the data. The method consists of a multi-stage analysis, including techniques for dividing texts into smaller so-called “meaning units” (MU). This division is not based on grammatical rules, but entirely on content which the researcher discovers and where there is a suitable shift of meaning. Thereafter the units are transformed so that the psychological and contextual implications are stressed making it possible to analyze the units when dealt with outside their original context. The analysis yielded 1,019 transformed meaning units that in turn generated 29 categories. Each category illustrated a special perspective of the phenomena studied and was described in a synopsis. To control for the reliability of the results of the study, the Norlander Credibility Test (NCT), designed for phenomenological analysis, was used (Åsenlöf, Olsson, Bood, & Norlander, 2007; Bergman & Norlander, 2005; Edebol, Bood, & Norlander, 2008; Janson, Archer, & Norlander, 2005). Two assessors then had the task of independently assigning 50 transformed MUs to 10 of the categories. The assessment of one of the assessors corresponded to 84%, while that of the other assessor reached 82%, yielding a mean of 83%. An additional NCT was done with two other independent assessors given the same data but with the instruction to place five MUs into each synopsis. The outcome was 80% for one of them and 88% for the other person, yielding a mean of 84%. Both of the results are in line with previously published results (Åsenlöf et al., 2007; Bergman & Norlander, 2005; Edebol et al., 2008; Janson et al., 2005). Finally, the material was transformed from “situated structures” into general themes or typological structures. This was done through a procedure whereby the three authors independently organized the synopses into general themes, then jointly compared their solutions (which were noticeably similar), and finally agreed on the themes.
Results and Discussion
As the analyses proceeded three themes emerged, each of which consisted of several categories: (a) The introduction of various sensorimotor exercises, (b) Regressions in terms of a return to earlier behavior, (c) Transformations in terms of positive development and change. The three themes emerged regularly throughout the entire study, and together they formed what is here called the kinesthetic-vestibular developmental model (see Figure 1).
The introductions are marked as points on the developmental curve and represent the new exercises provided at each return visit to the Institute. In the current study it was not possible to tell in advance how much time the client needed to fulfill the goal of training. Some needed longer to inhibit the primary reflexes while others matured more quickly. In accordance with the average return frequency, every eighth week, the model shows 16 introductions. The sensorimotor exercises push the process forward and create recurrent regressions (negative phases of development), in which three more distinct regressive periods can be discerned (R1 – R3). The periods are accompanied by positive phases of development where setbacks can be transformed into successes (T1 – T4). The kinesthetic-vestibular developmental curve, which was developed in the present study, is reminiscent of the traditional learning curve as described by, for example, Bachevalier and Mishkin (1984) and Fischer and Rose (2001). A similar curve was also developed by McGraw regarding physical development in prone position (Dalton, 1995). The development of both cognitive and bodily knowledge occurs in steps with plateaus as well as periods of setbacks (McGraw, 1995). The process of change assumed to accompany Retraining for Balance appears to produce accelerated development through regressions, thereby also improved conditions for learning. The instability and turbulence of the regressions are illustrated as wavy lines. Prigogine (1980), Varela (1999), and Ho (2005) described the flow similarly. In order to gain a more thorough understanding of the mechanisms of the process, each theme will first be discussed separately. Thereafter a discussion of the flow as a whole and an interpretation of the results will follow.
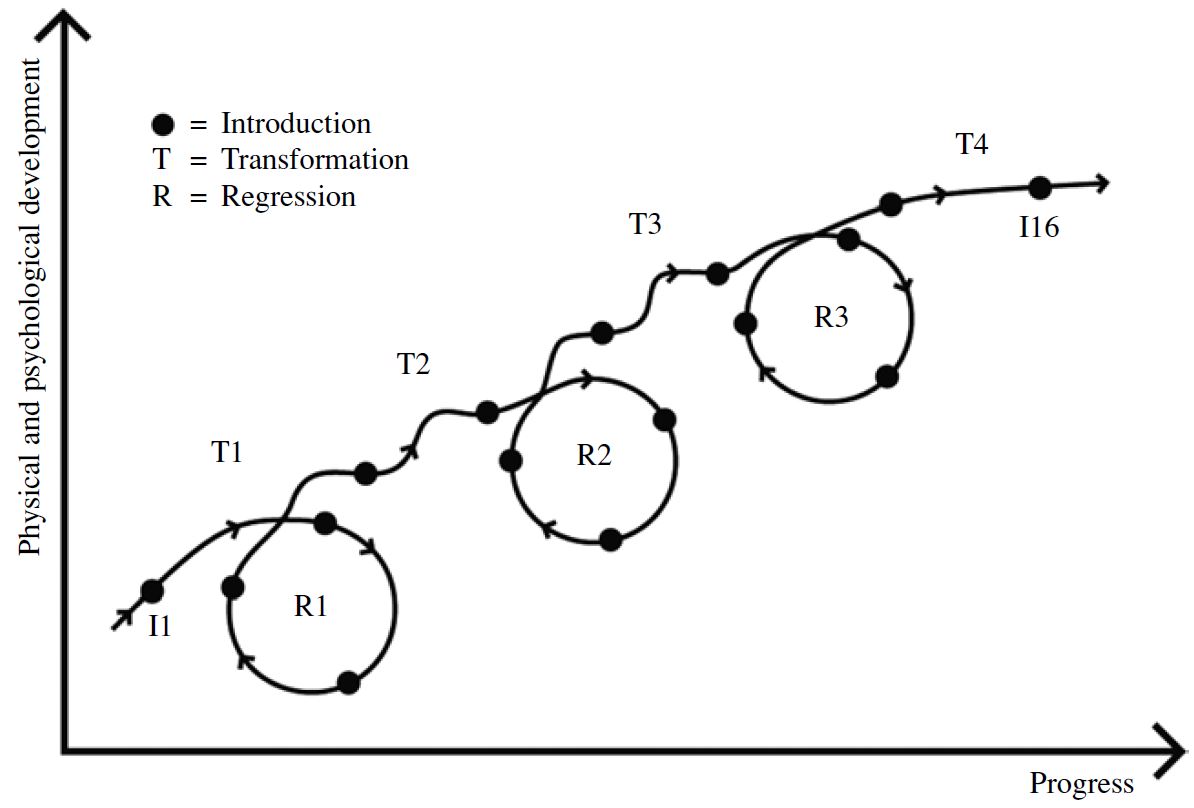
Figure 1. The participants needed close to 16 visits on average in order to complete the treatment in accordance with the sensorimotor therapy program Retraining for Balance. The visits (the introductions) are distributed along the curve above (I1-I16) and indicated as dots. During the treatment period three regression periods, here illustrated as circles (R1-R3), and four periods of transformation (T1-T4) were identified.
The Introductions
Starting treatment according to Retraining for Balance entailed new and regular routines for both children and parents. They were expected to jointly spend 15 minutes per day doing various exercises which at times could be both physically strenuous and mentally tiring as illustrated by the quotation: “when the fetal rock was repeated we immediately noticed that our child changed attitudes and started having peer problems”. At eight-week intervals the program at The Vestibularis Institute was modified, and children and parents were given the opportunity to discuss both successes and setbacks. New exercises were introduced in accordance with the sensorimotor maturity of each child as assessed on the tests (Niklasson & Niklasson, 1999, 2007) and in accordance with what the parents had experienced, in particular regarding the development of their child. The analysis of each individual flow chart indicated that when the training program was followed, then new exercises could be introduced largely similarly across clients. The training programs had two major elements. One was specific vestibular stimulation in which the client was first rocked in the arms of the mother and was then rotated on a rotating chair. The other consisted of stereotypic, vestibular, and kinesthetic infant movements. In both cases the children were blindfolded in order to maximally stimulate the vestibular system. Having the courage to shut out the external world and be left to oneself was a challenge at first but improved over time. During the first three introductions training consisted only of rocking in the arms of the mother. The exercise was perceived as something positive, but at times difficulties stretching, general bodily distress, yawning, and sometimes sweating were apparent. Despite the difficulties, it was common for the children to remind their parents and take the initiative to do the training, suggesting that the children felt the training was beneficial. At times the children resisted training. Often the resistance appeared when the children felt they were doing better, felt more secure, and felt they did not need further training. It also occurred during periods of defiance. The children’s fatigue also increased, resulting in a greater ability to go to sleep at night. Throughout the process the fatigue sometimes increased but at other times disappeared, and more energy was evident, “previously my child did not feel like doing anything at all. Now he wants to do everything.”
Regressions
During the training period physical and psychological regressions appeared continuously, but the analysis defined three periods of particular importance. Those periods were in the beginning (R1), in the middle (R2), and at the end of training (R3). Regardless of the children’s age at R1, R2, and R3, the parents felt that the behavior of the clients was similar in each period. R1 occurred in conjunction with the introductions 2, 3, and 4 and typically entailed that the younger children, especially at night, wet their pants and older children exhibited mood changes. Difficulties controlling the bladder occurred even before the first return visit in some cases, “my child started bed-wetting at night and it never happened before”. Even difficulties controlling the bowels occurred. Periodically such difficulties remained for a large part of the training period but disappeared, in most cases, upon completion of the training. R2, which occurred around the introductions 7, 8, and 9, primarily involved an increase in self-pity, sadness, and a wish to be with the mother. The children might cry and be sad without reason. The children who initially were angry and frustrated began to tend to whine during setbacks, “my child is sadder now. He used to be more aggressive”. The parents also noted that the children preferred to stay home in their room rather than being outside playing with peers. Favorite toys which had been discarded were once again desired for support and security. The need for proximity to his/her mother also increased during this time. Sibling rivalry and an insistence on fairness were evident. The increased sensitivity of the period remained periodically during training but had disappeared at the end of training. R3, which occurred around the introductions 12, 13, and 14, involved a great deal of defiance. The parents reported an increase in self-assertion and sometimes exaggerated self- confidence. Some children questioned issues that were self-evident and often the defiance was directed at the mother. One parent expressed the perception that “my child behaves like a teenager”. The behavior then diminished and was gone at the time of the completion of the training.
The analysis also indicated that across the training period additional regressions occurred. The regressions appeared more randomly and did not affect the developmental process in the same way. One example was that the children’s speech deteriorated periodically only to improve later, or they exhibited verbal tics such as onomatopoeic words which appeared and disappeared during the training period. Infant speech also appeared. An additional example was that the need to suck fingers and clothing intensified only to return to normal later. A wish to sleep together with the parents also increased during certain periods.
Transformations
The various periods of positive development and change, which emerged either following an introduction or following a period of regression, were labeled trans- formations. During those continuously recurrent periods sensorimotor skills as well as psychological abilities developed. For the large part the process change was gradual, suggesting that positive characteristics were slowly reinforced over time. Even before the first return visit, the participants exhibited a sense of calm and an improved ability to settle in the evening. “My son has calmed down and there are fewer outbursts”, one parent reported. Even when gross motor skills temporarily deteriorated, there were generally significant improvements.
In several cases the children showed a much greater interest in physical activity. When the children felt in control of their body, they enjoyed both physical education and sports outside school more. “My child participates more actively. He is not just present”. Some children occasionally felt a need for muscular exertion and then appeared to enjoy combat sports. When their legs cooperated, they found it easier to run and dribble, and soccer then became more attractive. Fine motor skill abilities also developed, facilitating writing and drawing.
Despite the fact that no specific oral motor training was offered, some children improved with regard to an ability to articulate along with the improvements in gross and fine motor skills. At the start of the training parents reported that difficulties with concentration were a significant problem. The analysis showed that the difficulties were transformed into an improved ability to concentrate, which in turn affected learning and the ability to generally deal with the school environment, “we have received great help both with regard to the language delay and the difficulties of concentration”. A reduction of restlessness and distress was also noted during the process of training. Periodically motor agitations negatively affected school work for some children, but upon completion of the training harmony and calm were evident. For some parents, reading problems and other learning difficulties were the reason for starting therapy. The analysis showed that academic proficiency improved although for some difficulties with mathematics remained, as seen in the quotation, “math is still fairly difficult. Other than that my son has met all goals in school”. As the children’s energy increased and their school work improved, homework improved as well. Some children started to have less trouble with play. Previously they had not engaged in role play and used to have difficulties playing with other children. During the training period their social skills and inventiveness improved. T4 resulted in such stability that both the instructor and the parents felt that the training process could be terminated. “Everything regarding our daughter now feels good. We are ready to go on”. One child said: “I feel the training has been good for me”.
Generalizability
The process involved in Retraining for Balance might be described as a flow in which Introductions, Regressions, and Transformations jointly pushed the individual toward an increased sensorimotor (physical) and psychological maturity. Introductions of kinesthetic and vestibular exercises initiated and sustained the processes that resulted in negative outcomes (regressions). What is meant by negative outcomes is a return to earlier sensorimotor (physical) and/or psychological behaviors which were then exercised. Engaging in earlier behaviors was at times perceived as demanding or strange by people in the surrounding environment. The negative developmental stages were then replaced by positive outcomes (transformations), where new behaviors perceived as more mature and age appropriate emerged.
In order to examine whether the results of the present study could be generalized to a larger group of children, the records of the eight participants were compared to the records of the remaining 224 children and adolescents from the earlier study of sensorimotor therapy (Niklasson et al., 2009). Two of the authors independently rated all records vis-à-vis the kinesthetic-vestibular model of development in terms of either “very good adjustment”, ”good adjustment”, or “doubtful or poor adjustment”. The results, which were noticeably alike, were then compared and agreed on. In order to meet the criteria for a “very good adjustment”, the records were required to clearly show the three regression periods (R1 – R3) and the four periods of transformation (T1 – T4). A “good adjustment” allowed for the omission of one of the regression periods, although the main tendency of the developmental curve had to be present. A “doubtful or poor adjustment” involved the presence of only one regression period and few transformations. The results indicated that 63% of the children and adolescents exhibited a “very good adjustment” to the kinesthetic model of development, whereas 32% of the records were judged to show a “good adjustment” to the model. Only 5% of the records (i.e., 11 children) were judged to show a “doubtful or poor” adjustment to the model. It is worth noting that the distribution above was obtained as early as when a third of the records had been assessed, suggesting that saturation had been reached (Hayes, 2004).
Conclusions
In general, the purpose of a qualitative study is to develop an understanding of what is going on (Hayes, 2004). Why? is never asked in a phenomenological study but answers are sought to questions such as how? and what? (Bergman & Norlander, 2005). In the analysis of the current study a number of psychological and physical phenomena emerged during periods of both regression and transformation. As mentioned in the introduction, the concept of regression has been defined in several different ways and in some cases the concept carried a negative connotation. The current analysis showed, with the aid of the EPP- method, that there was positive development following the reported regressions. Research from the Loeb Center for Nursing and Rehabilitation in New York has previously described similar results (Liedloff, 1986). Some regressions might appear extreme but, as mentioned above, clients often took the initiative to do the daily training which is interpreted as high motivation despite the efforts. When it comes to “regression in the service of the ego”, Kroebner (1963) suggested ‘Playfulness’ as a way to cope. Within the frames of Retraining for Balance, playfulness (Niklasson et al., 1999, 2007) as well as emotional understanding from surrounding grown-ups, especially the parents, is stressed (Erikson, 1987; Niklasson et al., 2009; Schilder, 1964, 1971). During the continuously recurrent periods of transformations, sensorimotor (physical) skills as well as psychological abilities developed. Findings which are in line with those gained by Levin (1991) and Jeannerod (1985, 2007). The phenomenological method has previously been of importance to psychology and psychiatry (Naudin et al., 1999) and has yielded knowledge about basic human characteristics such as a sense of time, a sense of being in the body, “embodiment”, and inter-subjectivity. Given this background, it is important to note Husserl (cited in Petit, 1999) and his observation that the young child possesses an internal drive toward an increased body control, and that such control is acquired through repetition, that is, movement makes the human self-constituting. Using the concept of self-cohesiveness, Levin (1991) speculates that the vestibulocerebellar-cortical system is of importance when it comes to the formation of early memories for further learning. According to van Gelder (1999), known patterns function as keys in a system which open up to recognition. Rothschild (2000) emphasized the ability of the body to store memories and the ability of the sensory systems to elicit them. The present study using the Retraining for Balance method might contribute to psychology and psychiatry by showing a novel way to reach ‘Winnicott’s third space’ (Winnicott, 1989). According to Bergström (1989, 1997) this “space” is similar to the limbic system as described by MacLean (1973). The limbic system is essential for successful bonding as well as for social and emotional behavior (Levin, 1991). The regressions identified in our analysis may be part of the “multitude” (manifold) of possible but not yet fully realized sensorimotor (physical) and psychological behaviors, which sometimes seem necessary for transformations (Ahrenfelt, 2001). This notion is in line with findings by Battegay (1970) who argued that regressions conceal a latent hope for the future.
While in qualitative studies validity is emphasized and while human beings are unique, phenomenological research findings are difficult to replicate (Hayes, 2004). However, viewed together with the results from a quantitative study on the same cohort a more thorough understanding ought to be reached. Results of the present study lead to the conclusion that an important reason for the positive development observed in the study of the 232 children and young people (Niklasson et al., 2009) may be that the body, through vestibular and kinesthetic stimulation, was given new possibilities to open up and recognize implicit/stored memories (Ogden, Minton, & Pain, 2006). An example might be a quotation from one of the children: “I am grieving my grandmother’s death” although she died many years ago. It appears as though memories from past developmental phases are elicited (R, negative change) through kinesthetic and vestibular stimulation (I), and in this way immature sensorimotor and psychological behaviors are given additional opportunities for realization, maturation, and development (T, positive change). Sensorimotor therapy, based on the kinesthetic-vestibular developmental model, might thus constitute a therapeutic complement to other types of treatment − for example, educational efforts, medication, and cognitive behavior therapy.
References
Adolph, K. E., Bertenthal, B. I., Boker, S. M., Goldfield, E. C., & Gibson, E. J. (1997). Learning in the development of infant locomotion. Monographs of the Society for Research in Child Development (Serial No. 251), 62(3), 1-162.
Ahrenfelt, B. (2001). Förändring som tillstånd [Change as a state of being]. Lund, Sweden: Studentlitteratur.
Arnold, L. E., Clark, D. L., Sachs, L. A., Jakim, S., & Smithies, C. (1985). Vestibular and visual rotational stimulation as treatment for attention deficit and hyperactivity. The American Journal of Occupational Therapy, 39, 84-91.
Åsenlöf, K., Olsson, S., Bood, S. Å., & Norlander, T. (2007). Case studies on fibromyalgia and burn-out depression using psychotherapy in combination with flotation-REST: Personality development and increased well-being. Imagination, cognition, and personality, 26, 259-271.
Bachevalier, J., & Mishkin, M. (1984). Learning and retention in infant monkeys. In M. H. Johnson (Ed.), Brain development and cognition: A reader (p. 198). Oxford, UK: Blackwell.
Bach-y-Rita, P. (2004). Is it possible to restore function with two percent surviving neural tissue? Journal of Integrative Neuroscience, 3, 3-6.
Balint, M. (1968). The basic fault: Therapeutic aspects of regression. Evanston, IL: Northwestern University Press.
Barnes, M., & Berke, J. (1991). En resa genom själens mörker [Two accounts of a journey through madness]. Stockholm: Nordstedts.
Battegay, R. (1970). Regressionsphänomene aus klinischer sicht unter besonderer berücksichtigung analytischer kurzpsychotherapie [Regression phenomena from the clinical viewpoint, with special consideration of analytic short therapy]. Praxis der Psychotherapie, 15, 151-162.
Bee, H. (1992). The developing child. New York: HarperCollins College Publishers.
Bergman, A., & Norlander, T. (2005). “Hay Sachs Anonymous”: Living in the shadow of the unidentified. Psychological aspects of physical inactivity from a phenomenological perspective. The Qualitative Report, 10, 795-816.
Bergström, R. M. (1969). An entropy model of the developing brain. Developmental Psychobiology, 2, 139-152.
Bergström, R. M. (1989). Meaning and the living brain. In P. Pylkkänen (Ed.), The search for meaning: The new spirit in science and philosophy. Wellingborough, UK: Crucible.
Bergström, R. M. (1997). Svarta och vita lekar [Black and white games]. Stockholm: Wahlström & Widstrand.
Berns, R. S. (1966). Regressive emotional behavior in college students. American Journal of Psychiatry, 122, 1378-1384.
Berthoz, A. (2000). The brain’s sense of movement. Cambridge, MA: Harvard University Press.
Brodal, A. (1981). Neurological anatomy in relation to clinical medicine. New York: Oxford University Press.
Brodal, P. (2004). The central nervous system: Structure and function. New York: Oxford University Press.
Capute, A. J., & Accardo, P. J. (1991). Developmental disabilities in infancy and childhood. Baltimore, MD: Paul Brooks.
Capute, A. J., Shapiro, B. K., Palmer, F. B., Accardo, P. J., & Wachtel, R. C. (1981). Primitive reflexes: A factor in nonverbal language in early infancy. In R. E. Stark (Ed.), Language behavior in infancy and early childhood (pp. 157-161). Amsterdam: Elsevier.
Dalton, T. C. (1995). McGraw’s alternative to Gesell’s maturationist theory. In T. C. Dalton & V. W. Bergenn (Eds.), Beyond heredity and environment. Myrtle McGraw and the maturation controversy. Boulder, CO: Westview Press.
Dennett, D. C. (1991). Consciousness explained. Boston, MA: Little, Brown & Co.
Dennett, D. C. (2003). Who’s on first? Heterophenomenology explained. Journal of Consciousness Studies, 10, 19-30.
Doidge, N. (2007). The brain that changes itself. New York: Viking.
Downing, G. (1997). Kroppen och ordet. Kroppsorienterad psykoterapi-teoretisk bakgrund och klinisk tillämpning [The body and the word. Body-orientated psychotherapy-theoretical background and clinical application]. Stockholm: Natur och Kultur.
Edebol, H., Bood, S. Å., & Norlander, T. (2008). Chronic whiplash-associated disorders and their treatment using flotation-REST (Restricted Environmental Stimulation Technique). Qualitative Health Research, 18, 480-488.
Erikson, E. (1987). Childhood and society. London: Paladin.
Field, J., & Blythe, P. (1989). Towards developmental re-education. Wichenford, UK: Field Educational Publications.
Fiorentino, M. R. (1981). Reflex testing methods for evaluating C.N.S development (Publ. No. 865). Springfield, IL: Charles C. Thomas Publisher Ltd.
Fischer, K. W., & Rose, L. T. (2001). Webs of skill: How students learn. Educational Leadership, 59, 6-12.
Freud, S. (1980). Orientering i psykoanalys [Introductory lectures on psychoanalyses]. Stockholm: Natur och Kultur.
Frick, S. M., & Hacker, C. (2001). Listening with the whole body. Madison, WI: Vital Links.
Gaines, R., & Missiuna, C. (2007). Early identification: Are speech/language-impaired toddlers at increased risk for Developmental Coordination Disorder? Child: Care, Health, and Development, 33, 325-32.
Gallagher, S. (1997). Mutual enlightenment: Recent phenomenology in cognitive science. Journal of Consciousness Studies, 4, 195-214.
Goddard, S. (2002). Reflexes, learning and behavior: A window into the child’s mind. Eugene, OR: Fern Ridge Press.
Goddard Blythe, S. (2005). Releasing educational potential through movement: A summary of individual studies carried out using the INPP test battery and developmental exercise programme for use in schools with children with special needs. Child Care in Practice, 11, 415-432.
Goddard Blythe, S., & Hyland, D. (1998). Screening for neurophysiological dysfunction in the specific learning difficulty child. The British Journal of Occupational Therapy, 61, 459-464.
Goldfield, E. C. (1989). Transitions from rocking to crawling: Postural constraints on infant movement. Developmental Psychology, 25, 913-919.
Guyton, A. C. (1991). Basic neuroscience: Anatomy and physiology. Philadelphia, PA: W. B. Saunders.
Haak, N. (1982). Allmän neuroslära på psykoanalytisk grund [General teachings in neurosis from a psychoanalytical point of view]. Stockholm: Natur och Kultur.
Halmagyi, G. M., Curthoys, I. S., Colebatch, J. G., & Aw, S. T. (2005). Vestibular responses to sound. In S. Ramat & D. Straumann (Eds.), Clinical and basic oculomotor research: In honor of David S. Zee (pp. 54-67). New York: New York Academy of Sciences.
Hayes, N. (2004). Doing psychological research. Maidenhead, UK: Open University Press.
Ho, M. W. (2005). The rainbow and the worm: The physics of organisms. London: World Scientific Publishing Co.
Holbech, B. P. (1986). Music recorded on audiocassette and CD. Bornholm, Denmark: Rotna Music.
Holle, B. (1985). Rörelseberedd-lekberedd? Praktisk vägledning i barns grovmotoriska utveckling [Ready to move – ready to play? A practical guide to children’s gross motor development]. Stockholm: Natur och Kultur.
Holt, K. S. (1991). Child development: Diagnosis and assessment. London: Butterworth- Heinemann.
Illingworth, R. S. (1987). The development of the infant and young child: Normal and abnormal. London: Churchill Livingstone.
Janson, L., Archer, T., & Norlander, T. (2005). The achievement of timing at the highest competitive level: The necessity of a ‘driving conviction’. Athletic Insight, 7(2). Retrieved August 6, 2005, from http://www.athleticinsight.com/Vol7Iss2/achievementofTiming.htm
Jeannerod, M. (1985). The brain machine: The development of neurophysiological thought. Cambridge, MA: Harvard University Press.
Jeannerod, M. (2007). Motor cognition: What actions tell the self. Oxford, UK: Oxford University Press.
Karlsson, G. (1995). Psychological qualitative research. Stockholm: Almqvist & Wiksell.
Kolb, B., & Whishaw, I. (1990). Fundamentals of human neuropsychology. New York: Freeman.
Kris, E. (1952). Psychoanalytic explorations in art. New York: International Universities Press.
Kroebner, T. C. (1963). The coping functions of the ego mechanisms. In R. W. White (Ed.), The study of lives: Essays on personality in honor of Henry A. Murray (pp. 178-198) New York: Atherton Press.
Levin, F. M. (1991). Mapping the mind: The intersection of psychoanalysis and neuroscience. Hillsdale, NJ: The Analytic Press, Inc.
Levine, P. A., & Frederick, A. (1997). Waking the tiger. Berkeley, CA: North Atlantic Books.
Liedloff, J. (1986). Kontinuumbegreppet [The continuum concept]. Stockholm: Carlsson Bokförlag.
Loewald, H. W. (1981). Regression: Some general considerations. Psychoanalytic Quarterly, 50, 22-43.
MacLean, P. (1973). A triune concept of the brain and behaviour. Toronto, Canada: The University of Toronto Press.
Maurer, D., & Maurer, C. (1989). The world of the newborn. London: Viking.
McFadden, D. (1993). A speculation about the parallel ear asymmetries and sex differences in hearing sensitivity and otoacoustic emissions. Hearing Research, 68, 143-151.
McGraw, M. B. (1995). General principles of growth. In T. C. Dalton & V. W Bergenn (Eds.), Beyond heredity and environment: Myrtle McGraw and the maturation controversy. Boulder, CO: Westview Press.
McPhillips, M., Hepper, P. G., & Mulhem, G. (2000). Effects of replicating primary-reflex movements on specific reading difficulties in children: A randomized, double-blind, controlled trial. The Lancet, 355, 537-541.
McPhillips, M., & Sheehy, N. (2004). Prevalence of persistent primary reflexes and motor problems in children with reading difficulties. Dyslexia: An International Journal of Research and Practice, 10, 316-338.
Morrison, D. C. (1985). Neurobehavioral and perceptual dysfunction in learning disabled children. Lewiston, NY: C. J. Hogrefe, Inc.
Naudin, J., Gros-Azorin, C., Mishara, A., Wiggins, O. P., Schwartz, M. A., & Azorin, J. M. (1999). The use of the Husserlian reduction as a method of investigation in psychiatry. Journal of Consciousness Studies, 6, 155-171.
Niklasson, M., & Niklasson, I. (1999). Retraining for Balance - Physiological Test. Mönsterås, Sweden: Vestibularis.
Niklasson, M., & Niklasson, I. (2007). Retraining for Balance - Physiological Test Revised. Mönsterås, Sweden: Vestibularis.
Niklasson, M., Niklasson, I., & Bergström, M. (1999). Retraining for Balance - Methods. Mönsterås, Sweden: Vestibularis.
Niklasson, M., Niklasson, I., & Bergström, M. (2007). Retraining for Balance - Methods Revised. Mönsterås, Sweden: Vestibularis.
Niklasson, M., Niklasson, I., & Norlander, T. (2009). Sensorimotor therapy: Using stereotypic movements and vestibular stimulation to increase sensorimotor proficiency of children with attentional and motor difficulties. Perceptual and Motor Skills, 108, 643-669.
Ogden, P., Minton, K., & Pain, C. (2006). Trauma and the body: A sensomotor approach to psychotherapy. New York: W. W. Norton & Company, Inc.
Okamoto, H., Stracke, H., Ross, B., Kakigi, R., & Pantev, C. (2007). Left hemispheric dominance during auditory processing in a noisy environment. BioMed Central Biology, 5, 52. https://doi.org.10.1186/1741-7007-5-52
Ornitz, E. M. (1983). Normal and pathological maturation of vestibular function in the human child. In R. Romand (Ed.), Development of auditory and vestibular systems. New York: Academic Press.
Paine, R. S., Brazelton, T. B., Donovan, D. E., Drorbaugh, J. E., Hubbell, J. P., & Sears E. M. (1964). Evolution of postural reflexes in normal infants and in the presence of chronic brain syndromes. Neurology, 14, 1036-1048.
Passer, M. W., & Smith, R. E. (2001). Psychology: Frontiers and applications. New York: McGraw- Hill Higher Education.
Petit, J. L. (1999). Constitution by movement: Husserl in light of recent neurobiological findings. In J. Petitot, F. J. Varela, B. Pachoud, & J. M. Roy (Eds.), Naturalizing phenomenology: Issues in contemporary phenomenology and cognitive science (pp. 220-244). Stanford, CA: Stanford University Press.
Pless, M. (2001). Developmental co-ordination disorder in pre-school children. Effects of motor skill intervention, parents’ descriptions, and short-term follow-up of motor status. Unpublished doctoral dissertation, Uppsala University, Sweden.
Prigogine, I. (1980). From being to becoming: Time complexity in the physical sciences. New York: Freeman.
Purves, D., Augustine, G. J., Fitzpatrick, D., Katz, L. C., LaMantia, A. S., & McNamara, J. O. (1997). Neuroscience. Sunderland, MA: Sinauer Associates, Inc.
Restak, R. M. (1980). The brain: The last frontier. New York: Warner Books, Inc.
Rintala, P., & Linjala, J. (2003). Scores on test of gross motor development of children with dysphasia: A pilot study. Perceptual and Motor Skills, 97, 755-762.
Robbins, J. (1977). Vestibular integration: Man’s connection to the earth. Somatics, 1, 27-36.
Rood, M. S. (1956). Neurophysiological mechanisms utilized in the treatment of neuromuscular dysfunction. American Journal of Occupational Therapy, 10, 220-225.
Rothschild, B. (2000). The body remembers. New York: W.W. Norton & Company.
Schilder, P. (1964). Contributions to developmental neuropsychiatry. New York: International Universities Press, Inc.
Schilder, P. (1971). Mind: Perception and thought in their constructive aspects. Freeport, New York: Books for Libraries Press.
Stern, D. N. (1985). The interpersonal world of the human infant. New York: Basic Books, Inc.
Stockmeyer, S. A. (1967). An interpretation of the approach of Rood to the treatment of neuromuscular dysfunction. American Journal of Physical Medicine, 46, 900-961.
Storr, A. (1993). Music and the mind. New York: Ballantine Books.
Thelen, E., & Fisher, D. M. (1983). The organization of spontaneous leg movements in newborn infants. Journal of Motor Behavior, 15, 353-377.
Thelen, E., & Smith, L. B. (1994). A dynamic systems approach to the development of cognition and action. Cambridge, MA: The MIT Press.
Van Gelder, T. (1999). Wooden iron? Husserlian phenomenology meets cognitive science. In J. Petitot, F. J. Varela, B. Pachoud, & J. M. Roy (Eds.), Naturalizing phenomenology: Issues in contemporary phenomenology and cognitive science (pp. 245-265). Stanford, CA: Stanford University Press.
Varela, F. J. (1999). The specious present: A neurophenomenology of time consciousness. In J. Petitot, F. J. Varela, B. Pachoud, & J. M. Roy (Eds.), Naturalizing phenomenology: Issues in contemporary phenomenology and cognitive science (pp. 266-314). Stanford, CA: Stanford University Press.
Vose, R. H. (1986). Agoraphobia. London: Faber & Faber.
Werner, H. (1957). The concept of development from a comparative and organismic point of view. In D. B. Harris (Ed.), The concept of development: An issue in the study of human behavior. Minneapolis, MI: University of Minnesota Press.
Wilson-Pauwels, L., Akesson, E. J., & Stewart, P. A. (1988). Cranial nerves: Anatomy and clinical comments. Philadelphia, PA: Decker.
Winnicott, D. W. (1989). Lek och verklighet [Playing and reality]. Stockholm: Natur och Kultur.
Winnicott, D. W. (1991). Människans natur [Human nature]. Ludvika, Sweden: Dualis förlag.
Adolph, K. E., Bertenthal, B. I., Boker, S. M., Goldfield, E. C., & Gibson, E. J. (1997). Learning in the development of infant locomotion. Monographs of the Society for Research in Child Development (Serial No. 251), 62(3), 1-162.
Ahrenfelt, B. (2001). Förändring som tillstånd [Change as a state of being]. Lund, Sweden: Studentlitteratur.
Arnold, L. E., Clark, D. L., Sachs, L. A., Jakim, S., & Smithies, C. (1985). Vestibular and visual rotational stimulation as treatment for attention deficit and hyperactivity. The American Journal of Occupational Therapy, 39, 84-91.
Åsenlöf, K., Olsson, S., Bood, S. Å., & Norlander, T. (2007). Case studies on fibromyalgia and burn-out depression using psychotherapy in combination with flotation-REST: Personality development and increased well-being. Imagination, cognition, and personality, 26, 259-271.
Bachevalier, J., & Mishkin, M. (1984). Learning and retention in infant monkeys. In M. H. Johnson (Ed.), Brain development and cognition: A reader (p. 198). Oxford, UK: Blackwell.
Bach-y-Rita, P. (2004). Is it possible to restore function with two percent surviving neural tissue? Journal of Integrative Neuroscience, 3, 3-6.
Balint, M. (1968). The basic fault: Therapeutic aspects of regression. Evanston, IL: Northwestern University Press.
Barnes, M., & Berke, J. (1991). En resa genom själens mörker [Two accounts of a journey through madness]. Stockholm: Nordstedts.
Battegay, R. (1970). Regressionsphänomene aus klinischer sicht unter besonderer berücksichtigung analytischer kurzpsychotherapie [Regression phenomena from the clinical viewpoint, with special consideration of analytic short therapy]. Praxis der Psychotherapie, 15, 151-162.
Bee, H. (1992). The developing child. New York: HarperCollins College Publishers.
Bergman, A., & Norlander, T. (2005). “Hay Sachs Anonymous”: Living in the shadow of the unidentified. Psychological aspects of physical inactivity from a phenomenological perspective. The Qualitative Report, 10, 795-816.
Bergström, R. M. (1969). An entropy model of the developing brain. Developmental Psychobiology, 2, 139-152.
Bergström, R. M. (1989). Meaning and the living brain. In P. Pylkkänen (Ed.), The search for meaning: The new spirit in science and philosophy. Wellingborough, UK: Crucible.
Bergström, R. M. (1997). Svarta och vita lekar [Black and white games]. Stockholm: Wahlström & Widstrand.
Berns, R. S. (1966). Regressive emotional behavior in college students. American Journal of Psychiatry, 122, 1378-1384.
Berthoz, A. (2000). The brain’s sense of movement. Cambridge, MA: Harvard University Press.
Brodal, A. (1981). Neurological anatomy in relation to clinical medicine. New York: Oxford University Press.
Brodal, P. (2004). The central nervous system: Structure and function. New York: Oxford University Press.
Capute, A. J., & Accardo, P. J. (1991). Developmental disabilities in infancy and childhood. Baltimore, MD: Paul Brooks.
Capute, A. J., Shapiro, B. K., Palmer, F. B., Accardo, P. J., & Wachtel, R. C. (1981). Primitive reflexes: A factor in nonverbal language in early infancy. In R. E. Stark (Ed.), Language behavior in infancy and early childhood (pp. 157-161). Amsterdam: Elsevier.
Dalton, T. C. (1995). McGraw’s alternative to Gesell’s maturationist theory. In T. C. Dalton & V. W. Bergenn (Eds.), Beyond heredity and environment. Myrtle McGraw and the maturation controversy. Boulder, CO: Westview Press.
Dennett, D. C. (1991). Consciousness explained. Boston, MA: Little, Brown & Co.
Dennett, D. C. (2003). Who’s on first? Heterophenomenology explained. Journal of Consciousness Studies, 10, 19-30.
Doidge, N. (2007). The brain that changes itself. New York: Viking.
Downing, G. (1997). Kroppen och ordet. Kroppsorienterad psykoterapi-teoretisk bakgrund och klinisk tillämpning [The body and the word. Body-orientated psychotherapy-theoretical background and clinical application]. Stockholm: Natur och Kultur.
Edebol, H., Bood, S. Å., & Norlander, T. (2008). Chronic whiplash-associated disorders and their treatment using flotation-REST (Restricted Environmental Stimulation Technique). Qualitative Health Research, 18, 480-488.
Erikson, E. (1987). Childhood and society. London: Paladin.
Field, J., & Blythe, P. (1989). Towards developmental re-education. Wichenford, UK: Field Educational Publications.
Fiorentino, M. R. (1981). Reflex testing methods for evaluating C.N.S development (Publ. No. 865). Springfield, IL: Charles C. Thomas Publisher Ltd.
Fischer, K. W., & Rose, L. T. (2001). Webs of skill: How students learn. Educational Leadership, 59, 6-12.
Freud, S. (1980). Orientering i psykoanalys [Introductory lectures on psychoanalyses]. Stockholm: Natur och Kultur.
Frick, S. M., & Hacker, C. (2001). Listening with the whole body. Madison, WI: Vital Links.
Gaines, R., & Missiuna, C. (2007). Early identification: Are speech/language-impaired toddlers at increased risk for Developmental Coordination Disorder? Child: Care, Health, and Development, 33, 325-32.
Gallagher, S. (1997). Mutual enlightenment: Recent phenomenology in cognitive science. Journal of Consciousness Studies, 4, 195-214.
Goddard, S. (2002). Reflexes, learning and behavior: A window into the child’s mind. Eugene, OR: Fern Ridge Press.
Goddard Blythe, S. (2005). Releasing educational potential through movement: A summary of individual studies carried out using the INPP test battery and developmental exercise programme for use in schools with children with special needs. Child Care in Practice, 11, 415-432.
Goddard Blythe, S., & Hyland, D. (1998). Screening for neurophysiological dysfunction in the specific learning difficulty child. The British Journal of Occupational Therapy, 61, 459-464.
Goldfield, E. C. (1989). Transitions from rocking to crawling: Postural constraints on infant movement. Developmental Psychology, 25, 913-919.
Guyton, A. C. (1991). Basic neuroscience: Anatomy and physiology. Philadelphia, PA: W. B. Saunders.
Haak, N. (1982). Allmän neuroslära på psykoanalytisk grund [General teachings in neurosis from a psychoanalytical point of view]. Stockholm: Natur och Kultur.
Halmagyi, G. M., Curthoys, I. S., Colebatch, J. G., & Aw, S. T. (2005). Vestibular responses to sound. In S. Ramat & D. Straumann (Eds.), Clinical and basic oculomotor research: In honor of David S. Zee (pp. 54-67). New York: New York Academy of Sciences.
Hayes, N. (2004). Doing psychological research. Maidenhead, UK: Open University Press.
Ho, M. W. (2005). The rainbow and the worm: The physics of organisms. London: World Scientific Publishing Co.
Holbech, B. P. (1986). Music recorded on audiocassette and CD. Bornholm, Denmark: Rotna Music.
Holle, B. (1985). Rörelseberedd-lekberedd? Praktisk vägledning i barns grovmotoriska utveckling [Ready to move – ready to play? A practical guide to children’s gross motor development]. Stockholm: Natur och Kultur.
Holt, K. S. (1991). Child development: Diagnosis and assessment. London: Butterworth- Heinemann.
Illingworth, R. S. (1987). The development of the infant and young child: Normal and abnormal. London: Churchill Livingstone.
Janson, L., Archer, T., & Norlander, T. (2005). The achievement of timing at the highest competitive level: The necessity of a ‘driving conviction’. Athletic Insight, 7(2). Retrieved August 6, 2005, from http://www.athleticinsight.com/Vol7Iss2/achievementofTiming.htm
Jeannerod, M. (1985). The brain machine: The development of neurophysiological thought. Cambridge, MA: Harvard University Press.
Jeannerod, M. (2007). Motor cognition: What actions tell the self. Oxford, UK: Oxford University Press.
Karlsson, G. (1995). Psychological qualitative research. Stockholm: Almqvist & Wiksell.
Kolb, B., & Whishaw, I. (1990). Fundamentals of human neuropsychology. New York: Freeman.
Kris, E. (1952). Psychoanalytic explorations in art. New York: International Universities Press.
Kroebner, T. C. (1963). The coping functions of the ego mechanisms. In R. W. White (Ed.), The study of lives: Essays on personality in honor of Henry A. Murray (pp. 178-198) New York: Atherton Press.
Levin, F. M. (1991). Mapping the mind: The intersection of psychoanalysis and neuroscience. Hillsdale, NJ: The Analytic Press, Inc.
Levine, P. A., & Frederick, A. (1997). Waking the tiger. Berkeley, CA: North Atlantic Books.
Liedloff, J. (1986). Kontinuumbegreppet [The continuum concept]. Stockholm: Carlsson Bokförlag.
Loewald, H. W. (1981). Regression: Some general considerations. Psychoanalytic Quarterly, 50, 22-43.
MacLean, P. (1973). A triune concept of the brain and behaviour. Toronto, Canada: The University of Toronto Press.
Maurer, D., & Maurer, C. (1989). The world of the newborn. London: Viking.
McFadden, D. (1993). A speculation about the parallel ear asymmetries and sex differences in hearing sensitivity and otoacoustic emissions. Hearing Research, 68, 143-151.
McGraw, M. B. (1995). General principles of growth. In T. C. Dalton & V. W Bergenn (Eds.), Beyond heredity and environment: Myrtle McGraw and the maturation controversy. Boulder, CO: Westview Press.
McPhillips, M., Hepper, P. G., & Mulhem, G. (2000). Effects of replicating primary-reflex movements on specific reading difficulties in children: A randomized, double-blind, controlled trial. The Lancet, 355, 537-541.
McPhillips, M., & Sheehy, N. (2004). Prevalence of persistent primary reflexes and motor problems in children with reading difficulties. Dyslexia: An International Journal of Research and Practice, 10, 316-338.
Morrison, D. C. (1985). Neurobehavioral and perceptual dysfunction in learning disabled children. Lewiston, NY: C. J. Hogrefe, Inc.
Naudin, J., Gros-Azorin, C., Mishara, A., Wiggins, O. P., Schwartz, M. A., & Azorin, J. M. (1999). The use of the Husserlian reduction as a method of investigation in psychiatry. Journal of Consciousness Studies, 6, 155-171.
Niklasson, M., & Niklasson, I. (1999). Retraining for Balance - Physiological Test. Mönsterås, Sweden: Vestibularis.
Niklasson, M., & Niklasson, I. (2007). Retraining for Balance - Physiological Test Revised. Mönsterås, Sweden: Vestibularis.
Niklasson, M., Niklasson, I., & Bergström, M. (1999). Retraining for Balance - Methods. Mönsterås, Sweden: Vestibularis.
Niklasson, M., Niklasson, I., & Bergström, M. (2007). Retraining for Balance - Methods Revised. Mönsterås, Sweden: Vestibularis.
Niklasson, M., Niklasson, I., & Norlander, T. (2009). Sensorimotor therapy: Using stereotypic movements and vestibular stimulation to increase sensorimotor proficiency of children with attentional and motor difficulties. Perceptual and Motor Skills, 108, 643-669.
Ogden, P., Minton, K., & Pain, C. (2006). Trauma and the body: A sensomotor approach to psychotherapy. New York: W. W. Norton & Company, Inc.
Okamoto, H., Stracke, H., Ross, B., Kakigi, R., & Pantev, C. (2007). Left hemispheric dominance during auditory processing in a noisy environment. BioMed Central Biology, 5, 52. https://doi.org.10.1186/1741-7007-5-52
Ornitz, E. M. (1983). Normal and pathological maturation of vestibular function in the human child. In R. Romand (Ed.), Development of auditory and vestibular systems. New York: Academic Press.
Paine, R. S., Brazelton, T. B., Donovan, D. E., Drorbaugh, J. E., Hubbell, J. P., & Sears E. M. (1964). Evolution of postural reflexes in normal infants and in the presence of chronic brain syndromes. Neurology, 14, 1036-1048.
Passer, M. W., & Smith, R. E. (2001). Psychology: Frontiers and applications. New York: McGraw- Hill Higher Education.
Petit, J. L. (1999). Constitution by movement: Husserl in light of recent neurobiological findings. In J. Petitot, F. J. Varela, B. Pachoud, & J. M. Roy (Eds.), Naturalizing phenomenology: Issues in contemporary phenomenology and cognitive science (pp. 220-244). Stanford, CA: Stanford University Press.
Pless, M. (2001). Developmental co-ordination disorder in pre-school children. Effects of motor skill intervention, parents’ descriptions, and short-term follow-up of motor status. Unpublished doctoral dissertation, Uppsala University, Sweden.
Prigogine, I. (1980). From being to becoming: Time complexity in the physical sciences. New York: Freeman.
Purves, D., Augustine, G. J., Fitzpatrick, D., Katz, L. C., LaMantia, A. S., & McNamara, J. O. (1997). Neuroscience. Sunderland, MA: Sinauer Associates, Inc.
Restak, R. M. (1980). The brain: The last frontier. New York: Warner Books, Inc.
Rintala, P., & Linjala, J. (2003). Scores on test of gross motor development of children with dysphasia: A pilot study. Perceptual and Motor Skills, 97, 755-762.
Robbins, J. (1977). Vestibular integration: Man’s connection to the earth. Somatics, 1, 27-36.
Rood, M. S. (1956). Neurophysiological mechanisms utilized in the treatment of neuromuscular dysfunction. American Journal of Occupational Therapy, 10, 220-225.
Rothschild, B. (2000). The body remembers. New York: W.W. Norton & Company.
Schilder, P. (1964). Contributions to developmental neuropsychiatry. New York: International Universities Press, Inc.
Schilder, P. (1971). Mind: Perception and thought in their constructive aspects. Freeport, New York: Books for Libraries Press.
Stern, D. N. (1985). The interpersonal world of the human infant. New York: Basic Books, Inc.
Stockmeyer, S. A. (1967). An interpretation of the approach of Rood to the treatment of neuromuscular dysfunction. American Journal of Physical Medicine, 46, 900-961.
Storr, A. (1993). Music and the mind. New York: Ballantine Books.
Thelen, E., & Fisher, D. M. (1983). The organization of spontaneous leg movements in newborn infants. Journal of Motor Behavior, 15, 353-377.
Thelen, E., & Smith, L. B. (1994). A dynamic systems approach to the development of cognition and action. Cambridge, MA: The MIT Press.
Van Gelder, T. (1999). Wooden iron? Husserlian phenomenology meets cognitive science. In J. Petitot, F. J. Varela, B. Pachoud, & J. M. Roy (Eds.), Naturalizing phenomenology: Issues in contemporary phenomenology and cognitive science (pp. 245-265). Stanford, CA: Stanford University Press.
Varela, F. J. (1999). The specious present: A neurophenomenology of time consciousness. In J. Petitot, F. J. Varela, B. Pachoud, & J. M. Roy (Eds.), Naturalizing phenomenology: Issues in contemporary phenomenology and cognitive science (pp. 266-314). Stanford, CA: Stanford University Press.
Vose, R. H. (1986). Agoraphobia. London: Faber & Faber.
Werner, H. (1957). The concept of development from a comparative and organismic point of view. In D. B. Harris (Ed.), The concept of development: An issue in the study of human behavior. Minneapolis, MI: University of Minnesota Press.
Wilson-Pauwels, L., Akesson, E. J., & Stewart, P. A. (1988). Cranial nerves: Anatomy and clinical comments. Philadelphia, PA: Decker.
Winnicott, D. W. (1989). Lek och verklighet [Playing and reality]. Stockholm: Natur och Kultur.
Winnicott, D. W. (1991). Människans natur [Human nature]. Ludvika, Sweden: Dualis förlag.
Table 1. Retraining for Balance: Summary
Figure 1. The participants needed close to 16 visits on average in order to complete the treatment in accordance with the sensorimotor therapy program Retraining for Balance. The visits (the introductions) are distributed along the curve above (I1-I16) and indicated as dots. During the treatment period three regression periods, here illustrated as circles (R1-R3), and four periods of transformation (T1-T4) were identified.
The research has followed the ethical standards of the World Medical Association declaration of Helsinki concerning Ethical Principles of Medical Research Involving Human Subjects. The authors acknowledge the excellent technical assistance of Bo Ahrenfelt
MD
in visualizing the kinesthetic- vestibular developmental model in Figure 1.
Appreciation is due to reviewers including
Martin McPhillips
PhD
School of Psychology
Queen&rsquo
s University
Belfast BT7 1NN
Northern Ireland
Torsten Norlander, Department of Psychology, Karlstad University, SE-651 88 Karlstad, Sweden. Phone: +46 54 7001178; Fax: +46 54 839165; Email: [email protected]