The affective personality: Its relation to quality of sleep, well-being and stress
Main Article Content
The aim in this study was to assess whether or not there is an association between different types of affective personality and sleep quality. Ninety-one individuals, of whom 50 were healthy and 41 were patients with stress-related problems, responded to the Positive and Negative Affect Scales (PANAS; Watson, Clark, & Tellegen, 1988), Sleep Quality (SQ; Gillberg, 2004) scale, Diurnal Type Scale (DTS; Thorsvall, Åkerstedt, 1980), Hospital Anxiety Depression Scale (HAD; Hermann, 1997), Life Orientation Test (LOT; Scheier, & Carver, 1985), Stress and Energy (SE; Kjellberg, & Iwanowski, 1989) scale, and sleep-related questions. Results indicated that self-actualizing individuals (high PA and low NA) reported the best sleep quality particularly in comparison to self-destructive individuals (low PA and high NA). Individuals with a low level of NA (self-actualizing and low affective individuals) reported less stress. The high affective individuals (high PA and high NA) reported high levels of stress, high anxiety, as well as the second best quality of sleep and a high degree of optimism and energy. The results suggests that individuals who display high positive affectivity, optimism, and a high level of energy achieve a better sleep quality, and that this phenomenon may be true even when these individuals experience high levels of stress.
Sleep, a state of altered consciousness in which the impact of external stimuli is significantly reduced, is important to the mental and physical health of all individuals (Åkerstedt, 2001; Morin, Rodrigue, & Ivers, 2003; Wheatley, 1997). The state of sleep creates a perceptual wall between consciousness and the external world (Dement & Vaughan, 2000). It is fair to assume that sleep involves an anabolic recovery (Åkerstedt, 2001; Åkerstedt & Kecklund, 2002; Dement &Vaughan, 2000; Theorell,2003; Wheatley, 1997) as opposed to catabolic wakefulness, which is destructive (Åkerstedt, 2001). Recovery is achieved through the activation of the immune system, blood sugar levels are maintained at relatively high levels, and – for example – growth hormones and testosterone are released (Theorell; Åkerstedt, & Kecklund). Sleep functions as the opposite and antagonist of stress (Åkerstedt, 2001). A reduced quality of sleep, including difficulties falling asleep, several instances of waking during the night, early awakening, fatigue, and dysphoria in the morning (Wheatley) are often associated with stress and a reduced quality of life (Morin, Rodrigue, & Ivers) and also are often the first indications of a burnout syndrome and stress (Åkerstedt, 2003), as well as anxiety and depression (Åkerstedt & Kecklund; Wheatley), and may precipitate chronic sleep difficulties (Åkerstedt, 2001; Åkerstedt & Kecklund, 2002; Drake, Roehrs, & Roth, 2003). Stress involves an activation of the body’s defense system in response to the individual’s own demands or those of the environment (Åkerstedt, 2001; Aldwin, 1994; Dotevall & Dotevall, 1988; Levi, 2000; Ursil, 1986). An individual can tolerate a significant amount of stress if s/he gets sufficient rest (Åkerstedt, 2003), whereas lack of sleep leads to increased stress (Åkerstedt & Kecklund, 2002; Partinen, 1994; Theorell, 2003; Wheatley, 1997). Individuals who do not experience stress enjoy a better quality of sleep (Theorell). Thus, there exist strong and significant associations between stressful situations and sleep difficulties (Morin, Rodrigue, & Ivers, 2003; Wheatley, 1997). Breaking the vicious cycle of stress – sleep difficulties – psychological problems would then imply an increased quality of life (Wheatley).
Dreams can be of a problem-solving and compensatory nature. The purpose of dreams is also to improve memory and to handle and process stress. Stress and strain often lead to increased dreaming in order to compensate for the destructive stress and wakefulness (Åkerstedt, 2001). Nightmares – anxiety-ridden dreams – are related to poor sleep quality (Åkerstedt, 2001).
Many attempts have been made to develop a questionnaire for the measurement of the circadian rhythm (Thorsvall & Åkerstedt, 1980). There are individuals who prefer to rise early in the morning and go to bed early (morning routines), and there are others who prefer to sleep late and retire late (evening routines) (Åkerstedt, 2001). The Diurnal Type Scale (DTS) is a new measurement instrument with good reliability and stability. Morning versus evening routines are associated with sleep quality such that individuals who retire early and rise early obtain better sleep quality as a result of people’s biological clock which is tuned to sleeping early in the night (Åkerstedt, 2001; Thorsvall & Åkerstedt, 1980). Individuals with depression and other psychological disturbances often demonstrate a disturbed circadian rhythm. To some extent, this fact can explain the disturbed sleep quality (Drake, Roehrs, & Roth, 2003; Ursil, 1986). Regularity is an intimate factor in the association between the circadian rhythm and sleep quality (Åkerstedt, 2001; Partinen, 1994).
Circadian rhythms and personality types have been examined in a number of studies (Thorsvall & Åkerstedt, 1980). Watson and Clark (1984) argued that positive affectivity is positively related to different social and biological rhythms including the circadian rhythm. Affect can be used as a term denoting both emotional states and emotions. A positive affectivity (PA) is characterized by high self-reported energy, satisfaction, and enjoyment (Melvin & Molloy, 2000), by happiness over a long time period and across different situations, enthusiasm, activity, and involvement (Agho, Price, & Mueller, 1992; Watson, Pennebaker, & Folger, 1987). Individuals with a high level of PA typically experience greater life satisfaction, self-esteem, and control (Costa & McRae, 1980; Varg, 1997; Watson & Clark, 1984) compared to those with a low level of PA.
Negative affectivity (NA) is characterized by dissatisfaction, apathy over a long time period and across different situations, and is significantly related to – and correlated with – stress (Brief, Burke, George, Robinson, & Webster, 1988; Spector & O’Connell, 1994; Watson & Clark, 1984; Watson, Pennebaker, & Folger, 1987), depression (Chen & Spector, 1991; Norlander et al., 2002) and anxiety (Chen & Spector; Spector & O’Connell) and, therefore, may be associated with sleep disturbances.
Wilson, Gullone, and Moss (1998) demonstrated that usually there is no significant correlation between positive and negative affectivity. Therefore, Norlanderet al. (2002) concluded that it was possible, at the level of the individual, to have different combinations of high or low PA and NA values. Norlander et al. combined the scales into a model with four affective personality types: self-actualizing with a high PA and low NA; high affective with a high PA and high NA; low affective with a low PA and low NA; and self-destructive with a low PA and high NA.
Both NA and PA affect a person’s experience of stress (Aldwin, 1994; Melvin & Molloy, 2000). Individuals with a self-actualizing affective personality experience the least stress and those with a self-destructive personality the most stress (Bood, Archer, & Norlander, 2004; Norlander, von Schedvin, & Archer, 2005) whereas the low affective personality type experiences the second lowest and the high affective type the second highest level of stress of the four affective personality types. With regard to the ability to recover from a traumatic event, in one study (Norlander et al., 2005) in which picket police and employees at grocery stores responded to the Posttraumatic Growth Inventory (Tedeschi & Calhoun, 1996), it was suggested that the high affective individuals not only recovered the best but that they also improved their levels of functioning. The self-actualizers, too, showed good recovery, whereas the low affective types reported a poorer quality of life and the self-destructive individuals did the most poorly. The relationship between anxiety and depression has been shown to be strongly associated with NA (Ahrens & Haaga, 1993) but less so with PA (Chang & Sanna, 2001). Depressed individuals tend to have a low PA (Ahrens & Haaga). Individuals with a low negative affectivity and a high positive affectivity (self-actualizing) tend to report greater psychological well-being, especially in comparison with individuals with a combination of high negative affectivity and low positive affectivity (self-destructive; Bood, Archer, & Norlander, 2004; Norlander et al., 2002).
Optimistic individuals handle stress, psychological, and physical illness better than do pessimistic people (Andersson, 1996; Scheier & Carver, 1985). Optimism is also positively related to high self-esteem (Chang & Sanna, 2001) and negatively related to depression and anxiety (Ahrens & Haaga, 1993). In earlier studies, individuals with a combination of low NA and high PA (self-actualizing) have been shown to exhibit a higher level of optimism in comparison with the other personality types, whereas individuals with high NA and low PA (self-destructive) show a low level of optimism (Bood, Archer, & Norlander, 2004).
Previous researchers have shown that high PA individuals exhibit greater energy (Costa & McCrae, 1980). In their research, Norlander et al. Archer (2002) showed that individuals with a high level of energy perform better than do those with a low level.
Since no researchers have examined the associations between affective personality types and different levels of sleep quality, one purpose in the current study was to explore the association between affective personality types and sleep quality. An additional purpose was to explore the representation of the different personality types among healthy individuals and patients with stress-related problems and possible interactions between affective personality types and stress-related problems.
Method
Participants
Of the 91 individuals in the study, 50 were healthy and 41 were patients with stress-related problems. The age distribution was such that 10% were younger than 30 years of age, 61.5% were between 31 and 50, and 28.5% were 51 years old or above. There were 74 women and 17 men. A chi-square analysis (goodness-of-fit, 5% level) revealed that the two sexes were proportionately distributed with regard to the two independent variables in the study group and affective personality type (see “Design” below). Additional analyses (chi-square goodness-of-fit, 5% level) showed no significant differences between healthy individuals and patients in the four affective personality groups. In addition, there were no significant differences (ps > .05) with regard to education and age concerning their affective personality (Kruskal-Wallis) and Group (Mann-Whitney).
Design
The study had two independent variables; affective personality (consisting of the four personality types: self-actualizing, high affective, low affective, and self-destructive) and group (healthy individuals and patients). The four personality types were derived from the PANAS (Watson, Clark, & Tellegen, 1988) through a procedure developed by Norlander et al. (2002). Through this procedure one group of 27 individuals was formed (14 healthy and 13 patients) with a self-destructive personality type, another group of 19 (12 healthy and 7 patients) with a low affective personality type, one group of 21 (11 healthy and 10 patients) with a high affective personality type, and finally one group of 24 participants (13 healthy and 11 patients) with a self-actualizing personality type. A number of dependent variables were present and were derived from several personality tests and sleep-related questions based on empirical findings reviewed in the introduction section of this study.
Instruments
PANAS – Positive Affect and Negative Affect Scale The PANAS (Kercher, 1992; Varg, 1997; Watson, Clark & Tellegen, 1988) yields information on degree of positive and negative affectivity. The instrument consists of 10 adjectives for positive affectivity (PA), and 10 adjectives for negative affectivity (NA). The adjectives in the test describe feelings and emotional states (Melvin & Molloy, 2000; Watson et al., 1988). The participants rate on a 5-point scale, from 1 = not at all, to 5 = very much, how they have felt lately. The scores on the positive and negative adjectives are summed separately to yield one PA and one NA value. The scales have been validated against several other scales frequently used in the area of psychopathology (Huebner & Dew, 1995). It has been shown that there is no significant correlation between positive and negative affectivity which is interpreted as an indication of divergent validity (Wilson et al., 1998).
Norlander et al. (2002) improved on the PANAS instrument by deriving four different personality types. This was achieved by dividing the results on the PA scale into two identical halves, one with high PA and one with low PA. The same procedure was used regarding the NA scale, yielding four different groups: low PA and high NA = self-destructive, low PA and low NA = low affective, high PA and high NA = high affective and finally high PA and low NA = self-actualizing. In the current study the distribution was based on the Swedish norm group for the PANAS instrument (N = 1010). Cut-off points for low PA = 35 or less, for high PA = 36 or above, for low NA = 17 or less, and finally for high NA = 18 or above.
SE – Stress and Energy The SE is a self-report rating scale concerning perceived stress and energy (Kjellberg & Iwanowski, 1989). It consists of two scales, yielding data on an individual’s perceived stress level and perceived energy level. The response alternatives are 5-point scales where 0 = not at all, and 5 = very much. Mean values are calculated. The perceived neutral point of the stress scale is 2.4 on the average and of the energy scale 2.7 (Kjellberg & Iwanowski, 1989). The instruments have been validated against studies of different types of strain in the work environment and have test-retest scores of 0.73 to 0.78 (Iwanowski, 1989; Kjellberg & Bolin, 1974; Kjellberg & Iwanowski, 1989).
HAD – Hospital Anxiety Depression Scale The HAD is a rating scale concerning degree of anxiety and depression, used in various published articles. It was constructed by Zigmond and Snaith (cited in Hermann, 1997), for use with physically ill people. It has since been revised to be used as a rating scale for anxiety and depression. The HAD yields data on a person’s quality of life. Its validity and reliability were examined by Hermann. The instrument consists of 14 statements with four response alternatives, ranging from positive to negative or vice versa. There are seven statements regarding anxiety and seven regarding depression.
LOT – Life Orientation Test The LOT is used to measure degree of optimism (Scheier & Carver, 1985). The LOT contains 12 statements, half positive and half negative. Four are filler items which are deleted from the coding. The response alternatives consist of a 5-point scale where 0 = not at all true and 4 = absolutely true. The scale has been used in a large number of studies concerned with health and personality psychology (Andersson, 1996). It has also been used in a study of psychological and physical well-being in the area of sports (Norlander & Archer, 2002). Parallel test reliability is reported to 0.76 and internal consistency to 0.76 (Scheier & Carver) and test-retest reliability to 0.75 (Norlander & Archer). The LOT is also regarded as having an adequate level of convergent and discriminant validity (Scheier & Carver), as demonstrated by correlation statistics and by using LISREL version 6 (r = 0.64).
DTS – Diurnal Type Scale The DTS (Thorsvall & Åkerstedt, 1980) is used to measure an individual’s circadian rhythm, that is, “morning person”, “evening person”, or “neither morning nor evening person” on a 1-4 scale. Of its seven items, three concern the morning, three concern the evening, and one concerns both. The average response on the items is computed (Thorsvall & Åkerstedt). Morning people are those at 3 or above, evening people at 2 or below. Those whose scores are between these values are considered “neither, nor” (Åkerstedt et al.). In the current study, the mean for the patient group was M = 2.47, SD = 0.59 and the healthy group M = 2.44, SD = 0.57. The DTS has shown high internal reliability (Cronbach’s α = 0.75). The correlation coefficient for the norm group was r = 0.79 (p < .001) (Thorsvall & Åkerstedt, 1980). The DTS has been developed through a procedure where two dimensions may be studied (Gillberg, 2004), one index for the morning questions and one for the evening questions and these two were used in the current study.
SQ – Sleep Quality The sleep questions were first constructed for high school students (Gillberg, 2004). The 11 questions tap the sleeping habits of the participants, such as “At what time do you usually wake up on week days?”, “How often do you feel tired on week days?”, “How often do you feel tired/alert on week days?”, “How often do you feel tired in the morning/before lunch/after work on week days?” “What is usually your emotional state in the morning?”, “How often do you feel you did not get enough sleep?”, “How do you feel you usually sleep?”. Responses to nine of the questions are given on 0-4 scales, to one question on a 0-5 scale, and lastly to one question on a 0-8 scale. A few changes were made for the current study, such as statements concerning school were changed to work since the participants were working. In order to examine whether the 11 questions concerning quality of sleep could be summed, an inter-item correlation was computed (standardized item alpha = 0.88) which then allowed for summation. Thus, when the scores were summed, they ranged from 0 to 49.
Dream questions Two questions concerned with the participants’ dream habits were also in the questionnaire. They tapped nightmares and the number of nights the individual remembered dreaming.
Procedure
Two groups of participants were recruited. The participants in the patient group were randomly chosen among 150 patients with stress-related problems who volunteered and indicated an interest in Float-Rest at the Human Performance Laboratory in the Department of Psychology at the university. The questionnaire was mailed to the patient group and returned after two weeks in the envelope provided. The healthy group received the questionnaire at a conference at the Public Health Department. The participants in the healthy group were randomly selected among the approximately 130 people present at the conference and returned the questionnaire after two weeks to a designated person in the department. In order to ensure anonymity, the questionnaires were returned in sealed envelopes. It is worth noting that no person high in the hierarchy of the department could discern who returned an envelope.
Of the 100 questionnaires distributed, the response rate was 91%. All healthy individuals returned the questionnaire and 41 in the patient group. After one and one half weeks, a reminder was sent to the healthy group by email which reduced the attrition. A comparison of the questionnaires from individuals responding without a reminder and from individuals responding after the reminder was sent out (18 participants) did not indicate different characteristics in the responses. The patient group received no reminder since the response rate was considered good. A few questionnaires were returned after the deadline and were omitted from the analyses.
Results
Dependent Variables
A Pillai’s multivariate analysis of variance (MANOVA; 4 × 2 factorial design) was conducted with affective personality and group as independent variables and with sleep quality (SQ), morning routines (DTS), evening routines (DTS), nightmares, dream memories, anxiety (HAD), depression (HAD), positive affectivity (PANAS), negative affectivity (PANAS), stress (SE), energy (SE), and optimism (LOT) as dependent variables. The analysis yielded significant effects for affective personality (p < .001, Eta2 = 0.50, power = 0.99) and for group (p = .029, Eta2 = 0.29, power = 0.90), but not the interaction (p = .229, Eta2 = 0.16, power = 0.95). The results from the univariate F tests concerning affective personality and group are given below.
Sleep quality There was a significant difference with regard to group [F(1, 83) = 10.92, p = .001] where a descriptive analysis indicated that the patient group experienced poorer sleep quality (M = 22.77, SD = 8.79) compared to the healthy group (M = 27.88, SD = 6.52). There was also a significant effect for affective personality [F(3, 83) = 7.10, p < .001] and a post hoc test (Tukey’s highly significant differences, 5% level) showed that the self-actualizing individuals experienced a better sleep quality (M = 30.42, SD = 6.63) than did the self-destructive (M = 21.53, SD = 7.06). The remaining groups fell in between, (high affective: M = 25.91, SD = 9.43; low affective, M = 24.84, SD = 6.06). In order to explore whether or not the order of the means, self-actualizing–high affective–low affective–self-destructive, could be considered a statistically significant trend regarding sleep quality, a test of trends was performed (Joncheere Test for Ordered Alternatives; Siegel & Castellan, 1988). The result indicated that there was such a trend (J* = 3.51, p < .001).
Morning routines There was no significant difference for group (p = .925). There was, however, a significant effect for affective personality [F (3, 83) = 3.07, p = 0.032], and a post hoc test (Tukey’s HSD, 5% level) showed that the self-actualizing individuals displayed more morning routines (M = 3.02, SD = 0.58) than did the self-destructive (M = 2.40, SD = 0.82). The remaining groups fell in between, (high affective: M = 2.63, SD = 0.91: low affective: M = 2.45, SD = 0.74).
Evening routines There was no significant difference with regard to group (p = .239) nor with regard to affective personality (p = .695).
Nightmares There was no significant difference with regard to group (p = .142). There was, however, a significant effect for affective personality [F(3, 83) = 3.44, p = 0.021] and a post hoc test (Tukey’s HSD, 5% level) indicated that the high affective reported a higher frequency of nightmares (M = 2.29, SD = 0.78) than did the self-actualizing (M = 1.67, SD = 0.56). The remaining groups fell in between (low affective: M = 2.16, SD = 0.83; self-destructive: M = 2.07, SD = 0.68).
Dream memories There was no significant difference with regard to either group (p = .776) or affective personality (p = .301).
Anxiety There was a significant difference with regard to group [F(1, 83) = 5.73, p = .019] where a descriptive analysis showed that the patient group experienced more (M = 7.10, SD = 3.73) compared to the healthy group (M = 5.50, SD = 3.05). There was also a significant effect for affective personality [F(3, 83) = 14.79, p < .001] and a post hoc test (Tukey’s HSD, 5% level) showed that the self-actualizing experienced less anxiety (M = 3.46, SD = 2.19) compared to the self-destructive (M = 8.59, SD = 2.87) and the high affective (M = 7.01, SD = 3.21), whereas the low affective (M = 5.48, SD = 3.15) fell in between.
Depression There was no significant difference with regard to group (p = .077). There was, however, a significant effect for affective personality [F(3, 83) = 12.92, p < .001] and a post hoc test (Tukey’s HSD, 5% level) showed that the self-destructive reported more depression (M = 5.85, SD = 2.76) compared to the other groups (low affective: M = 3.19, SD = 2.69; high affective: M = 2.84, SD = 1.84; self-actualizing: M = 2.04, SD = 1.88).
Positive and Negative Affectivity As expected, there were significant results with regard to affective personality (p < .001). With regard to group there was no such effect for negative affectivity (p = .273) but for positive affectivity [F(1, 83) = 4.35, p = .040], where a descriptive analysis showed that the healthy group exhibited greater positive affectivity (M = 35.31, SD = 5.94) compared to the patient group (M = 33.60, SD = 8.18).
Stress There was no significant difference with regard to group (p = .620). There was, however, a significant effect for affective personality [F(3, 83) = 13.16, p < .001] and a post hoc test (Tukey’s HSD, 5% level) showed that the self-actualizing individuals (M = 1.49, SD = 0.83) and the low affective (M = 1.80, SD = 0.80) reported that they experienced less stress than did those who were high affective (M = 2.72, SD = 1.05) and self-destructive (M = 2.81, SD = 0.79).
Energy There was no significant difference with regard to group (p = .413). There was, however, a significant effect for affective personality [F(3, 83) = 16.21, p < .001] where a post hoc test (Tukey’s HSD, 5% level) indicated that the high affective (M = 3.81, SD = 0.64) and the self-destructive (M = 3.76, SD = 0.64) were more energetic than the low affective (M = 3.22, SD = 0.52) and the self-destructive (M = 2.65, SD = 0.85).
Optimism There was a significant difference with regard to group [F(1, 83) = 10.41, p = .002], where a descriptive analysis indicated that the healthy group experienced greater optimism (M = 22.93, SD = 4.21) compared to the patient group (M = 20.43, SD = 4.30). There was a significant effect for affective personality [F(3, 83) = 7.70, p < .001], and a post hoc test (Tukey’s HSD, 5% level) indicated that the self-actualizing (M = 24.38, SD = 3.88) and the high affective (M = 22.61, SD = 4.71) were more optimistic compared to the low affective (M = 21.18, SD = 3.69) and the self-destructive (M = 19.32, SD = 3.78).
Factor Analysis
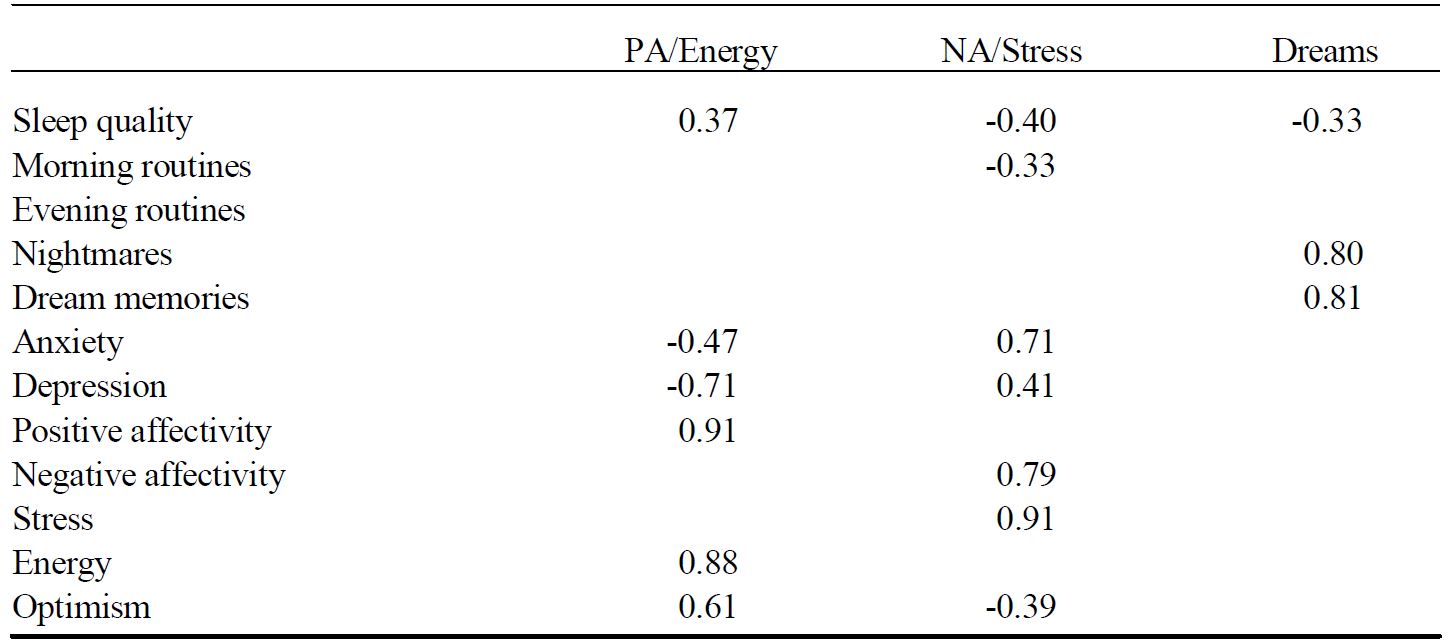
In order to further examine the associations among personality variables and sleep variables, an exploratory factor analysis (principal components analysis) with affective personality and the dependent variables was conducted. The Scree plot test indicated three factors (explained variance: 69.76 %) presented in Table 1.
Table 1. Factor Analysis (PCA) with the Dependent Variables of the Study. Method of Rotation: Varimax (Kaiser Normalization). Values Less Than 0.30 are Suppressed
Note: Kaiser normalization = Brace, Kemp, and Sneglar (2001)
Discussion
The current study was exploratory and no specific hypotheses were formulated. It was not surprising, however, that – compared to the healthy group – the patient group exhibited poorer health and sleep quality, greater anxiety, lower positive affectivity, and less optimism. It was more surprising, however, that the distribution of affective personality types was even between the two groups and that there were no interactions between personality and group. In other words, in the healthy group and the patient group the same relationships existed between personality types and the dependent variables, although the patients had poorer health. In addition, affective personality was shown to be of great importance to perceived health. It is possible to conclude that affective personality appears to be a basic and relatively stable personality trait not easily affected by diminished health, but with a strong influence on a series of health-related variables such as sleep quality, circadian rhythm, depression, stress, energy, and dispositional optimism.
The first of the three factors of the factor analysis represented positive affectivity, energy, optimism, and good sleep quality. This result is consistent with previous studies suggesting that sleep quality, energy, and optimism are positively intercorrelated (Thorsvall & Åkerstedt, 1980), as are positive affectivity, energy, and optimism (Bood et al., 2004). The current study showed that self-actualizing individuals (high PA and low NA) reported the best sleep quality, particularly in comparison to self-destructive individuals (low PA and high NA). A test of trends yielded a continuum regarding affective personality and sleep quality (self-actualizing–high affective–low affective–self-destructive). It appears that high positive affectivity is a more important component than either high or low negative affectivity when it comes to good sleep and its related good-health affects. This notion is underscored by the fact that the patients had lower positive affectivity than the healthy group did, whereas the groups did not differ in terms of negative affectivity.
The second factor of the factor analysis was characterized by negative affectivity, stress, depression, anxiety, late morning routines, and poor sleep quality, in line with several studies showing associations among stress, psychological problems, and reduced sleep quality (Morin, Rodrigue, & Ivers, 2003; Wheatley, 1997). The self-actualizing and low affective individuals reported less stress compared to the high affective and the self-destructive individuals, a finding which is consistent with earlier studies (Bood et al., 2004; Norlander et al., 2005). The fact that individuals with a low level of NA (the self- actualizing and low affective individuals) reported less stress suggests that low NA is a more important component compared to both high and low PA when it comes to the experience of lower stress levels. It has been shown that poorer sleep quality leads to increased stress (Åkerstedt & Kecklund, 2002; Partinen, 1994; Wheatley, 1997). This study indicated, however, that the reverse is not self-evident: high affective individuals reported high levels of stress, high anxiety, and the highest frequency of nightmares as well as the second best quality of sleep, and a high degree of optimism and energy!
The third factor of the factor analysis indicated that nightmares and dream memories are connected to poor sleep quality which is consistent with earlier studies (Åkerstedt, 2001) and was an expected result.
The notion of the participants with both high affectivity and a good sleep quality may be an example of how individuals with high stress levels who also exhibit high positive affectivity, optimism and energy, under favorable circumstances may develop coping strategies for mastering stressful situations thereby achieving a good quality of life and good sleep. Future researchers will have to determine whether all high affective individuals have the ability to transform stress into something beneficial and what mechanisms are involved in successful or less successful coping. In conclusion, our results in the current study suggest that individuals who display a positive attitude toward life (as assessed by positive affectivity and optimism) and a high level of energy achieve a better sleep quality, and that this phenomenon is true even when these individuals experience high levels of stress.
References
Agho, A. O., Price, J. L., & Mueller, C. W. (1992). Discriminant validity of measures of job satisfaction, positive affectivity and negative affectivity. Journal of Occupational and Organizational Psychology, 65, 185-196.
Ahrens, A. H., & Haaga, D. A. F. (1993). The specificity of attributional style and expectations to positive and negative affectivity, depression, and anxiety. Cognitive Therapy and Research, 17, 83-99.
Åkerstedt, T. (2001). Sömnens betydelse för hälsa och arbete. [The importance of sleep to health and work]. Järvsö, Sweden: Bauer Bok.
Åkerstedt, T. (2003). Den som sover är vaken. [To be asleep is to be awake]. Utveckla.Nu, 4, 20-21.
Åkerstedt, T., & Kecklund, G. (2002). Sömn och återhämtning [Sleep and recovery]. In R. Ekman & B. Arnetz (Eds.), Stress-molekylerna, individen, organisationen, samhället [The stress molecules, the individual, the organization, and society] (pp. 264-271). Stockholm: Liber.
Aldwin, C. (1994). Stress, coping and development. An interactive perspective. New York: Guilford.
Andersson, G. (1996). The benefits of optimism: A meta-analytic review of the Life Orientation Test. Personality and Individual Differences, 21, 719-725.
Bood, S. Å., Archer, T., & Norlander, T. (2004). Affective personality in relation to general personality, self-reported stress, coping and optimism. Individual Differences Research, 2, 26-37.
Brace, N., Kemp, R., & Sneglar, R. (2001). SPSS for psychologists. New York: Palgrave.
Brief, A. P., Burke, M, J., George, J. M., Robinson, B. S., & Webster, J. (1988). Should negative affectivity remain an unmeasured variable in the study of job stress? Journal of Applied Psychology, 73, 193-198.
Chang, E. C., & Sanna, L. J. (2001). Optimism, pessimism, and positive and negative affectivity in middle-aged adults: A test of a cognitive-affective model of psychological adjustment. Psychology and Aging, 16, 524-531.
Chen, P. Y., & Spector, P. E. (1991). Negative affectivity as the underlying cause of correlations between stressors and strains. Journal of Applied Psychology, 76, 398-407.
Costa, P. T., Jr., & McCrae, R. (1980). Influence of extroversion and neuroticism on subjective well-being: Happy and unhappy people. Journal of Personality and Social Psychology, 38, 668-687.
Dement, W. C., & Vaughan, C. (2000). The promise of sleep. New York: Dell.
Dotevall, G., & Dotevall, S. (1988). Hälsa och stress: Stress och sjukdom. Stockholm: Almqvist & Wiksell.
Drake, C. L., Roehrs, T., & Roth, T. (2003). Insomnia causes, consequences, and therapeutics: An overview. Depression and Anxiety, 18, 163-176.
Hermann, C. (1997). International experiences with the Hospital Anxiety and Depression Scale-A review of validation data and clinical results. Journal of Psychosomatic Research, 42, 17-41.
Huebner, E. S., & Dew, T. (1995). Preliminary validation of the positive and negative affect schedule with adolescents. Journal of Psycho-educational Assessment, 13, 286-293.
Iwanowski, S. (1989). Utprovning av adjektivchecklistan. Enheten för psykofysiologi [Testing the adjective checklist. Unit of psychophysiology]. Solna, Sweden: Arbetsmiljöinstitutet.
Kercher, K. (1992). Assessing, subjective well-being in the old-old: The PANAS as a measure of orthogonal dimensions of positive and negative affect. Research on Aging, 14, 131-168.
Kjellberg, A., & Bolin, B. (1974). Self-reported arousal: Further development of a multifactorial inventory. Scandinavian Journal of Psychology, 15, 285-292.
Kjellberg, A., & Iwanowski, S. (1989). Stress/Energi- formuläret: Utveckling av en metod för skattning av sinnesstämning i arbetet [The Stress-Energy questionnaire: Construction of a method for the assessment of mood states at work]. Solna, Sweden: Arbetsmiljöinstitutet, Undersökningsrapport.
Levi, L. (2000). Stress och hälsa 2000. Stockholm. Skandia.
Melvin, G. A., & Molloy, G, N. (2000). Some psychometric properties of the positive and negative affect schedule among Australian youth. Psychological Reports, 86, 1209-1212.
Morin, C. M., Rodrigue, S., & Ivers, H. (2003). Role of stress, arousal, and coping skills in primary insomnia. Psychosomatic Medicine, 65, 259-267.
Norlander, T., & Archer, T. (2002). Predicting performance outcome in ski and swim championships: Effectiveness of mood, perceived exertion and dispositional optimism. Perceptual and Motor Skills, 94, 153-164.
Norlander, T., Bood, S. Å., & Archer, T. (2002). Performance during stress: Affective personality, age, and regularity of physical exercise. Social Behavior and Personality: An international journal, 30, 495-508.
Norlander, T., von Schedvin, H., & Archer, T. (2005). Thriving as a function of affective personality: Relation to personality factors, coping strategies and stress. Manuscript submitted for publication.
Partinen, M. (1994). Sleep disorders and stress. The Journal of Psychosomatic Research, 38, 89-91.
Scheier, M. F., & Carver, C. S. (1985). Optimism, coping, and health: Assessment and implications of generalized outcome expectancies. Health Psychology, 4, 219-247.
Siegel, S., & Castellan, N. J. (1988). Nonparametric statistics for the behavioral sciences. New York: McGraw-Hill.
Spector, P. E., & O’Connell, B. J. (1994). The contribution of personality traits, affectivity, locus of control and Type A to the subsequent reports of job stressors and job strains. Journal of Occupational and Organizational Psychology, 67, 1-11.
Tedeschi, R. G., & Calhoun, L. G. (1996). The posttraumatic growth inventory: Measuring the positive legacy of trauma. The Journal of Traumatic Stress, 9, 455-471.
Theorell, T. (2003). Psykosocial miljö och stress. [The psychosocial environment and stress]. Lund, Sweden: Studentlitteratur.
Thorsvall, L., & Åkerstedt, T. (1980). A Diurnal Type Scale. Construction, consistency and validation in shift work. Scandinavian Journal of Work Environment Health, 6, 283-290.
Ursil, R. (1986). Sömn och sömnrubbningar. [Sleep and sleep disturbances]. Lund, Sweden: Naturoch Kultur.
Varg, N. (1997). Negativ affektivitets inverkan på svarsbeteende i enkätformulär. [The influence on negative affectivity on responses to survey questionnaires]. Stockholm: Stockholm University.
Watson, D., & Clark, L. (1984). Negative affectivity: The disposition to experience aversive negative stress. Psychological Bulletin, 96, 465-490.
Watson, D., Clark, L., & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect. The PANAS scale. Journal of Personality and Social Psychology, 54, 1063-1070.
Watson, D., Pennebaker, J. W., & Folger, R. (1987). Beyond negative affectivity: Measuring stress and satisfaction in the workplace. Journal of Organizational Behavior Management, 8, 141-157.
Wheatley, D. (1997). Stress, anxiety and depression. Stress Medicine, 13, 173-177.
Wilson, K., Gullone, E., & Moss, S. (1998). The youth version of the positive and negative affect schedule: A psychometric validation. Behavior Change, 15, 187-193.
Agho, A. O., Price, J. L., & Mueller, C. W. (1992). Discriminant validity of measures of job satisfaction, positive affectivity and negative affectivity. Journal of Occupational and Organizational Psychology, 65, 185-196.
Ahrens, A. H., & Haaga, D. A. F. (1993). The specificity of attributional style and expectations to positive and negative affectivity, depression, and anxiety. Cognitive Therapy and Research, 17, 83-99.
Åkerstedt, T. (2001). Sömnens betydelse för hälsa och arbete. [The importance of sleep to health and work]. Järvsö, Sweden: Bauer Bok.
Åkerstedt, T. (2003). Den som sover är vaken. [To be asleep is to be awake]. Utveckla.Nu, 4, 20-21.
Åkerstedt, T., & Kecklund, G. (2002). Sömn och återhämtning [Sleep and recovery]. In R. Ekman & B. Arnetz (Eds.), Stress-molekylerna, individen, organisationen, samhället [The stress molecules, the individual, the organization, and society] (pp. 264-271). Stockholm: Liber.
Aldwin, C. (1994). Stress, coping and development. An interactive perspective. New York: Guilford.
Andersson, G. (1996). The benefits of optimism: A meta-analytic review of the Life Orientation Test. Personality and Individual Differences, 21, 719-725.
Bood, S. Å., Archer, T., & Norlander, T. (2004). Affective personality in relation to general personality, self-reported stress, coping and optimism. Individual Differences Research, 2, 26-37.
Brace, N., Kemp, R., & Sneglar, R. (2001). SPSS for psychologists. New York: Palgrave.
Brief, A. P., Burke, M, J., George, J. M., Robinson, B. S., & Webster, J. (1988). Should negative affectivity remain an unmeasured variable in the study of job stress? Journal of Applied Psychology, 73, 193-198.
Chang, E. C., & Sanna, L. J. (2001). Optimism, pessimism, and positive and negative affectivity in middle-aged adults: A test of a cognitive-affective model of psychological adjustment. Psychology and Aging, 16, 524-531.
Chen, P. Y., & Spector, P. E. (1991). Negative affectivity as the underlying cause of correlations between stressors and strains. Journal of Applied Psychology, 76, 398-407.
Costa, P. T., Jr., & McCrae, R. (1980). Influence of extroversion and neuroticism on subjective well-being: Happy and unhappy people. Journal of Personality and Social Psychology, 38, 668-687.
Dement, W. C., & Vaughan, C. (2000). The promise of sleep. New York: Dell.
Dotevall, G., & Dotevall, S. (1988). Hälsa och stress: Stress och sjukdom. Stockholm: Almqvist & Wiksell.
Drake, C. L., Roehrs, T., & Roth, T. (2003). Insomnia causes, consequences, and therapeutics: An overview. Depression and Anxiety, 18, 163-176.
Hermann, C. (1997). International experiences with the Hospital Anxiety and Depression Scale-A review of validation data and clinical results. Journal of Psychosomatic Research, 42, 17-41.
Huebner, E. S., & Dew, T. (1995). Preliminary validation of the positive and negative affect schedule with adolescents. Journal of Psycho-educational Assessment, 13, 286-293.
Iwanowski, S. (1989). Utprovning av adjektivchecklistan. Enheten för psykofysiologi [Testing the adjective checklist. Unit of psychophysiology]. Solna, Sweden: Arbetsmiljöinstitutet.
Kercher, K. (1992). Assessing, subjective well-being in the old-old: The PANAS as a measure of orthogonal dimensions of positive and negative affect. Research on Aging, 14, 131-168.
Kjellberg, A., & Bolin, B. (1974). Self-reported arousal: Further development of a multifactorial inventory. Scandinavian Journal of Psychology, 15, 285-292.
Kjellberg, A., & Iwanowski, S. (1989). Stress/Energi- formuläret: Utveckling av en metod för skattning av sinnesstämning i arbetet [The Stress-Energy questionnaire: Construction of a method for the assessment of mood states at work]. Solna, Sweden: Arbetsmiljöinstitutet, Undersökningsrapport.
Levi, L. (2000). Stress och hälsa 2000. Stockholm. Skandia.
Melvin, G. A., & Molloy, G, N. (2000). Some psychometric properties of the positive and negative affect schedule among Australian youth. Psychological Reports, 86, 1209-1212.
Morin, C. M., Rodrigue, S., & Ivers, H. (2003). Role of stress, arousal, and coping skills in primary insomnia. Psychosomatic Medicine, 65, 259-267.
Norlander, T., & Archer, T. (2002). Predicting performance outcome in ski and swim championships: Effectiveness of mood, perceived exertion and dispositional optimism. Perceptual and Motor Skills, 94, 153-164.
Norlander, T., Bood, S. Å., & Archer, T. (2002). Performance during stress: Affective personality, age, and regularity of physical exercise. Social Behavior and Personality: An international journal, 30, 495-508.
Norlander, T., von Schedvin, H., & Archer, T. (2005). Thriving as a function of affective personality: Relation to personality factors, coping strategies and stress. Manuscript submitted for publication.
Partinen, M. (1994). Sleep disorders and stress. The Journal of Psychosomatic Research, 38, 89-91.
Scheier, M. F., & Carver, C. S. (1985). Optimism, coping, and health: Assessment and implications of generalized outcome expectancies. Health Psychology, 4, 219-247.
Siegel, S., & Castellan, N. J. (1988). Nonparametric statistics for the behavioral sciences. New York: McGraw-Hill.
Spector, P. E., & O’Connell, B. J. (1994). The contribution of personality traits, affectivity, locus of control and Type A to the subsequent reports of job stressors and job strains. Journal of Occupational and Organizational Psychology, 67, 1-11.
Tedeschi, R. G., & Calhoun, L. G. (1996). The posttraumatic growth inventory: Measuring the positive legacy of trauma. The Journal of Traumatic Stress, 9, 455-471.
Theorell, T. (2003). Psykosocial miljö och stress. [The psychosocial environment and stress]. Lund, Sweden: Studentlitteratur.
Thorsvall, L., & Åkerstedt, T. (1980). A Diurnal Type Scale. Construction, consistency and validation in shift work. Scandinavian Journal of Work Environment Health, 6, 283-290.
Ursil, R. (1986). Sömn och sömnrubbningar. [Sleep and sleep disturbances]. Lund, Sweden: Naturoch Kultur.
Varg, N. (1997). Negativ affektivitets inverkan på svarsbeteende i enkätformulär. [The influence on negative affectivity on responses to survey questionnaires]. Stockholm: Stockholm University.
Watson, D., & Clark, L. (1984). Negative affectivity: The disposition to experience aversive negative stress. Psychological Bulletin, 96, 465-490.
Watson, D., Clark, L., & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect. The PANAS scale. Journal of Personality and Social Psychology, 54, 1063-1070.
Watson, D., Pennebaker, J. W., & Folger, R. (1987). Beyond negative affectivity: Measuring stress and satisfaction in the workplace. Journal of Organizational Behavior Management, 8, 141-157.
Wheatley, D. (1997). Stress, anxiety and depression. Stress Medicine, 13, 173-177.
Wilson, K., Gullone, E., & Moss, S. (1998). The youth version of the positive and negative affect schedule: A psychometric validation. Behavior Change, 15, 187-193.
Table 1. Factor Analysis (PCA) with the Dependent Variables of the Study. Method of Rotation: Varimax (Kaiser Normalization). Values Less Than 0.30 are Suppressed
Note: Kaiser normalization = Brace, Kemp, and Sneglar (2001)
This study was supported by grants from the County Council (Landstinget)
Vä
rmland (LiV)
Sweden. Appreciation is due to reviewers including
Girardin Jean-Louis
Box 58
SUNY Downstate Medical Center
450 Clarkson Avenue
Brooklyn
NY 11203-2098
USA. Email