Thriving in adversity: Do life skills programs work for developing world children? A pragmatic randomized controlled trial
Main Article Content
The severe adversity experienced by millions of children in the developing world leads to failure to thrive associated with cognitive deficits, emotional management problems, and social impairment. In this pragmatic randomized controlled trial, 909 children (aged 8–15 years) in India with disadvantaged backgrounds took part in a semistructured program involving sports or creative arts activities. The Life Skills Assessment Scale was used to assess the children’s life skills before and after taking part in the program. Children who took part in the program showed significant increases in life skills following participation, compared to a control group. This study demonstrates the impact of simple, low-budget programs on cognitive, emotional, and social life skills that are typically delayed by severe adversity. The findings have clear implications for children in other adverse environments, such as conflict zones and settlements for displaced children resulting from war, natural disasters, and emergency events.
Even with the rapid increase in the middle classes, millions of children in the developing world experience damaging poverty and adversity, leading to severe disruption to normal development, including failure to thrive and stunted growth (de Onis & Branca, 2016). Regardless of culture or geography, children’s physical growth is assessed as normal in a predetermined way by measurement on an appropriate growth chart; stunted growth can be defined as a child being at least two standard deviations below the expected median (de Onis & Branca, 2016).
As statutory services are not available for the majority of the children experiencing poverty and adversity, many thousands of nongovernmental organizations (NGOs) run programs designed to ameliorate these effects. Most of the NGOs rely on volunteers, very small budgets, and anecdotal or “common sense” evaluations rather than standardized measures of effectiveness (Sawhill & Williamson, 2001). The impact of these interventions remains unclear.
Literature Review
The Problem
Global levels of child poverty are not known or defined precisely. Estimates suggest that 40–47% of children survive on less than the equivalent of USD 2.00 per day, equating to millions of children living in absolute poverty globally (Olinto et al., 2013; United Nations International Children’s Emergency Fund, 2016; World Bank Group, 2018). The Hunger and Malnutrition Survey estimated that the growth of up to 59% of children under 5 years of age in India was stunted (Naandi Foundation, 2012). Similar figures were reported by the Indian Ministry of Statistics and Program Implication (2012). Although a rapid decline in the number of children with stunted growth had been seen in previous decades, in the National Family Health Survey-4, India (World Bank Group, 2018) it was found that these improvements have stalled. This appears to be a common picture across much of the developing world, with the problem compounded by increasing numbers of displaced children (Save the Children’s Resource Centre, 2017; World Bank Group, 2018). Chronic malnutrition among those aged under 5 years, as measured by stunted growth, is estimated to affect 37.0% of children in sub-Saharan Africa (Woldehanna et al., 2017), 47.0% of children in Kenya (Bloss et al., 2004), 31.4% of children in Western Africa, and 38.3% of children in Oceania (United Nations International Children’s Emergency Fund, World Health Organization, & World Bank Group, 2017). Similar figures have been reported in the Philippines (Mendez & Adair, 1999) and Zimbabwe (Alderman et al., 2006).
Severe child adversity comes in many forms, including poor nutrition, physical or sexual abuse, living in a war zone, being displaced, being in institutional care, and receiving poor or dysfunctional parenting. The negative effects of climate change have also been recognized as having a greater impact on those with fewer (vs. more) economic resources (Mendelsohn et al., 2006). Daniel et al. (2010) described child adversity as “the experience of life events and circumstances which may combine to threaten or challenge healthy development” (p. 105). The weight of empirical evidence now irrefutably links severe adversity (usually caused by poverty) to deficits in child development and long-term mental health issues (see, for brief reviews, Kennedy et al., 2013; Read & Bentall, 2012). In addition to the impact on children’s physical growth, the psychological effects of severe adversity in childhood can be grouped as shown in Table 1.
Although many studies have focused on very young children and found associations between stunted growth and poor cognitive, social, and emotional outcomes, these effects can be long-term or even lifelong (Alderman et al., 2006; Brown & Pollitt, 1996; Pollitt et al., 1993; Victora et al., 2008). Hoddinott et al. (2013) found that stunted growth at 72 months predicted deficits in attention and memory, and information-processing problems in reading and nonverbal cognitive skills at 25 years, resulting in “diminished learning capacity and poor school performance” (United Nations International Children’s Emergency Fund, 2009, p. 16), and “a lifetime of lost opportunities in education” (Save the Children’s Resource Centre, 2017, p. 8). Thus, to minimize long-term adverse effects, interventions are required that target older children and young adults, not just the very young.
Table 1. Psychological Effects of Severe Childhood Adversity and Failure to Thrive
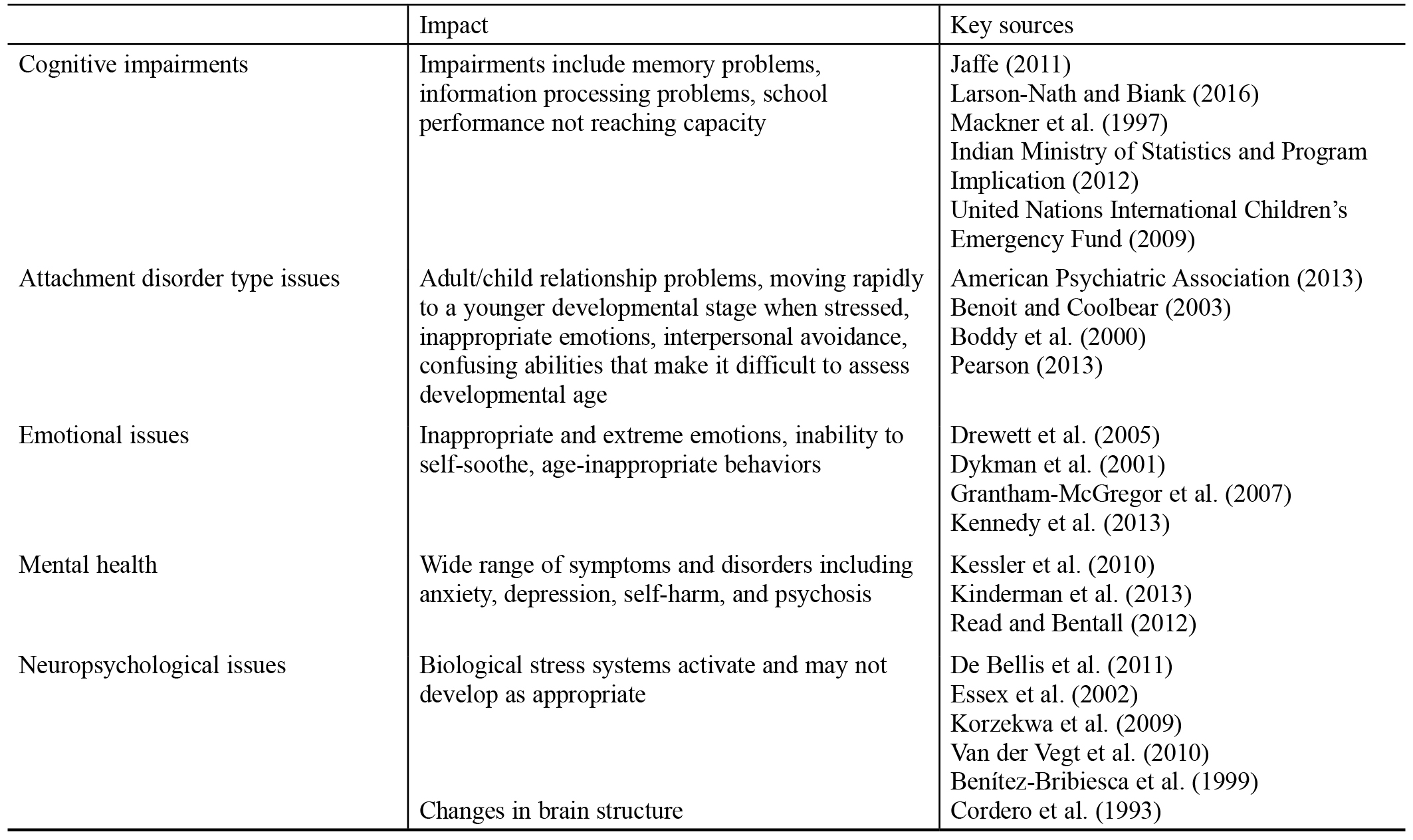
Note. Adapted from Pearson et al. (2020).
Symptoms Versus Life Skills
The effects of severe early adversity can be described in terms of symptoms or life skills. This decision point is generally culturally based. Although a simplification, in the Western world, failure to thrive is typically considered symptomatic of a medical or developmental disorder, often diagnosed as organic/nonorganic. By contrast, conceptualizing life skills problems highlights the practical nature of what children need to thrive given the demands of the 21st century. The World Health Organization described life skills as “skills that support psychosocial competence or performance (the ability of an individual to deal effectively with demands or challenges of everyday life). It is the ability to maintain a person’s well-being and to show it in adaptable and positive behaviors when interacting with other people, their culture and environment” (cited in Birrell et al., 1997, p. 5). These skills have been categorized by the United Nations International Children’s Emergency Fund (2009) into three areas: cognitive skills, personal skills, and interpersonal skills. Development of each area is essential for self-management, personal development, and the ability to communicate effectively with others. Similar classifications have been described by Ceylan and Gök Çolac (2019), who used the categories of self-awareness (of feelings, values, and strengths), self-management (regulating emotions, stress, and impulses), and social awareness (including empathy).
Nongovernment Organization Responses
More than three million NGOs operate in India, with a large proportion working with underprivileged children; the actual number is not known because of the lack of registration requirements (Mahapatra, 2014). Many programs run by these NGOs aim to ameliorate the impact of early adversity on children’s development. However, there is little empirical evidence that these programs are effective. Various interventions are run, including provision of nutrition and physical care, enrichment activities, vocational skills programs, mentoring, and life skills training. Enrichment programs are typically semistructured social interventions, commonly involving sports and creative arts activities that enable children to interact with others and to experience and practice life skills in a safe and nonjudgmental setting, with adult facilitators. The programs typically include some discussion about the life skills used during the activity to help children understand and learn to apply these effectively. These programs tend to be low budget (or funding free) and do not require specialist facilitation.
The Current Study
In our pragmatic controlled trial conducted in Bengaluru, India, we used the Life Skills Assessment Scale (LSAS; Kennedy et al., 2014), which is a standardized measure, to assess empirically whether an NGO enrichment program focused on sports and creative arts improved children’s life skills. We predicted that participants in the intervention group would show greater improvements in life skills compared with participants in the control group.
Method
Participants
We analyzed data from 1,244 participants who were observed and assessed in the study, comprising 909 children aged between 8 and 15 years who took part in the programs, and 335 children aged between 8 and 15 years who were in the Fun Days control group.
Procedure
Children in the intervention group took part in semistructured enrichment sessions involving sports or creative arts activities at the low-cost or free school that they attended as students. Low-cost and free schools provide basic education accessed by families with a low economic status, including those living in slums. The staff at the schools had previously arranged for their school to partner with the host NGO, but had not yet started the partnership. None of the schools nor any of the children had previously taken part in an enrichment-type program. Sessions took place during school time and ran once per week for 2–3 hours each session. Each child attended 25 weekly sessions as part of the normal school curriculum. Children chose a sports or creative arts program in which to participate until sessions reached their maximum numbers of 20–30 students. Sessions were explicitly socially inclusive, with no separation by gender, religion, or socioeconomic group, and were structured as follows:
a) Check in and introductions
b) Short warm-up game or exercises (e.g., singing songs with accompanying actions, yoga stretches)
c) A sport (football) or creative arts (visual, drama, dancing) activity
d) Structured discussion and reflection on what was observed and learned during the activity
e) Wrap-up game incorporating “thank you” and “goodbye”
The control group comprised of children who took part in Fun Day sessions offered by the host NGO to schools or groups of children who are not currently partners for programs. The control group schools were matched for economic, social, and religious profiles with the program group, and both groups were assessed by the same observer/raters. After the final Fun Day sessions, participating schools were offered the opportunity to become partner organizations with the host NGO, with a view to providing regular input. Fun Days included games (e.g., passing balloons to teammates standing in rows, team running exercises) but no debriefing or reflection to consolidate skills.
Observers/raters assessed the children at the start of the session and again after the 25 sessions were complete, about 6 months later. Over a period of 3 weeks, 11 observers attended the first three of each of the sports and creative arts sessions, dividing the groups of children between them. Each observer rated approximately 15 children over three sittings, each lasting 2 hours. Each child’s initial LSAS rating was recorded using tablet computers, and this procedure was repeated at the end of the program from weeks 23 to week 25. Children were not necessarily assessed in the same order at the start and the end of the program. Initial scores for the control group were collected during the Fun Days. Again, each observer assessed around 15 individual children at a time. The length of time available to observe each child was comparable for the intervention and control groups, that is, 6 hours at the start and the same time again after 25 weeks.
Table 2. Gender and Age of Participants by Group

Measure
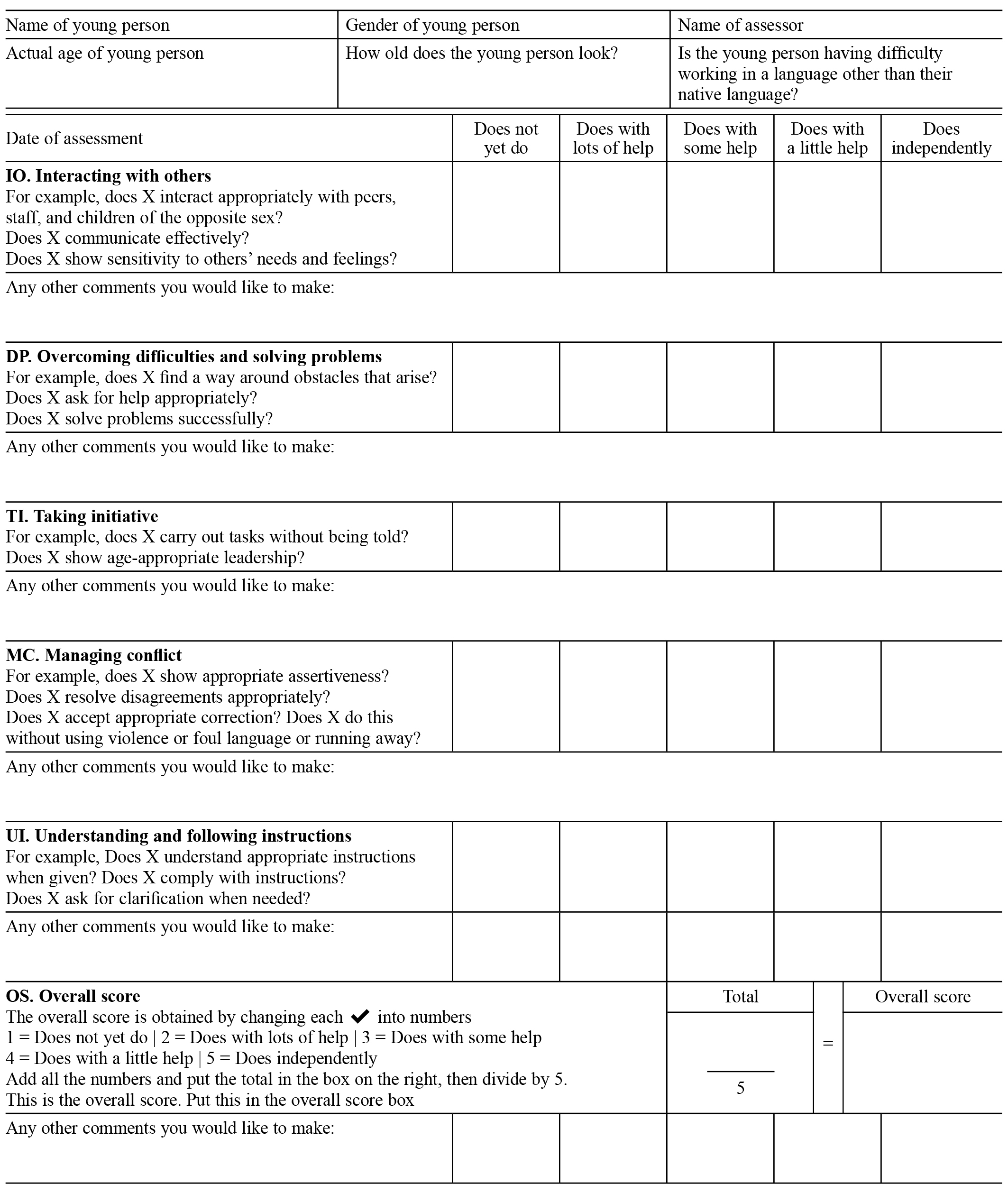
The LSAS (Kennedy et al., 2014) is a five-item, observer-rated, standardized scale designed to assess the life skills of disadvantaged children in the developing world (see Appendix), and it is in widespread use (e.g., Mandigo et al., 2018). In a similar way that simple standardized assessments are currently used to assess child development, each of the five LSAS items assess wider dimensions of life skills:
a) Interacting with others
b) Overcoming difficulties and solving problems
c) Taking initiative
d) Managing conflict
e) Understanding and following instructions
The LSAS was initially standardized for three age groups: 8–10 years, 11–13 years, and 14–16 years (Kennedy et al., 2014), and more recently for young adults aged 17–19 years and 20–22 years (Pearson et al., 2020). The LSAS has good interrater reliability (r = .88, p < .01), internal consistency reliability (α = .86), and test–retest reliability (r = .86) for each age group (Kennedy et al., 2014). Each item is assessed using a 5-point Likert type scale: 1 = does not yet do, 2 = does with lots of help, 3 = does with some help, 4 = does with a little help, 5 = does independently. To encourage the observer to move away from pass/fail type judgement, the rating numbers do not appear on the scoring sheet; instead, these are added after the initial assessment is complete. An overall (average) score for each child is obtained by adding up the scores and dividing by 5. The development and application of the LSAS is covered in detail in Kennedy et al. (2014) and Pearson et al. (2020).
Observers/Raters
All 11 observers/raters (six women and five men) worked for local NGOs. Some had come from disadvantaged backgrounds themselves, and some had attended enrichment programs as children. The observers/raters did not participate in the programs being assessed. All of them attended a brief orientation session regarding the purpose and administration of the LSAS. They were not made aware of the research objective.
Ethical Considerations
An independent steering group considered the study and discussed ethical issues raised. It was decided that all parts of the study, including the control group activities, were comparable to normal organization activities. Fun Day sessions are routinely offered at the schools where the control group’s data were collected. Informed consent was obtained from participating partners.
Results
Descriptive Statistics
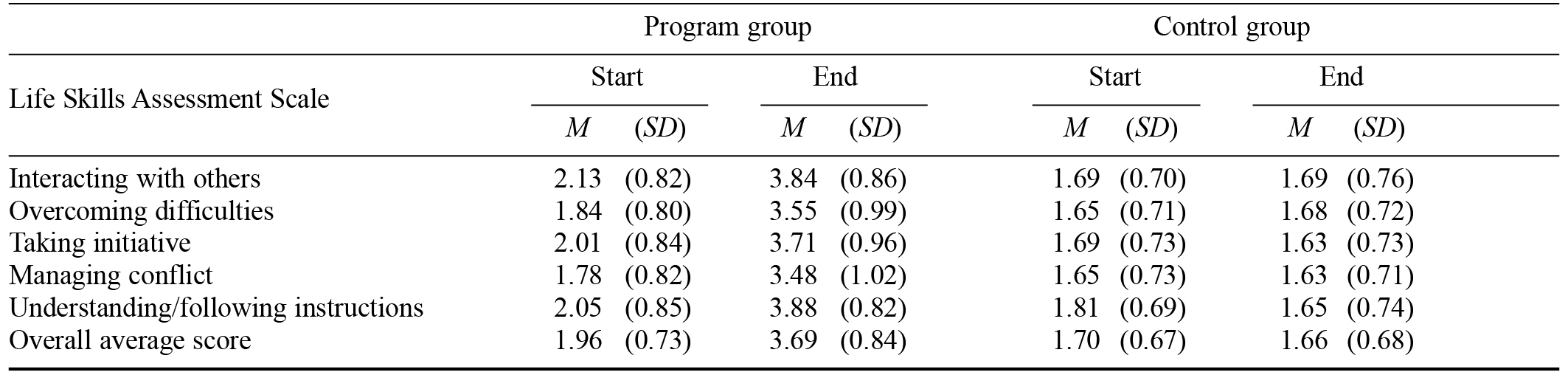
Table 3 and Figure 1 illustrate the mean LSAS scores at the start and end of the study period for the program and control groups.
Table 3. Descriptive Statistics for the Life Skills Assessment Scale Scores
Group Comparisons
We used SPSS version 24 to inspect the distribution of data and calculate descriptive statistics. The data were compared for any initial differences between the two groups using chi-square analysis for gender and t tests for age and initial LSAS score. There were no group differences in gender, χ2(1, 1244) = 2.05, p = .15, although there were slight group differences in both age, t(1242) = 6.17, p < .001 (see Table 2), and life skills, t(1242) = 5.76, p < .001 (see Table 3) at the start of the study.
A mixed-model analysis of variance (ANOVA) was used to assess the impact of the program, with one within-subjects factor (time: preprogram vs. postprogram) and one between-subjects factor (group: intervention vs. control). Although the LSAS data were not normally distributed, ANOVAs are sufficiently robust to accommodate some deviation from the norm, and so the original analysis plan was retained. The ANOVA results show that there were main effects of group, F(1, 1242) = 1207.19, p < .001, ηp2 = 0.49; time, F(1, 1242) = 563.60, p < .001, ηp2 = 0.31; and the group × time interaction, F(1, 1242) = 616.47, p < .001, ηp2 = 0.33. Life skills increased considerably over time in the intervention group, t(908) = 44.21, p < .001, and did not change in the control group, t(334) = –0.78, p = .44 (see Figure 1).
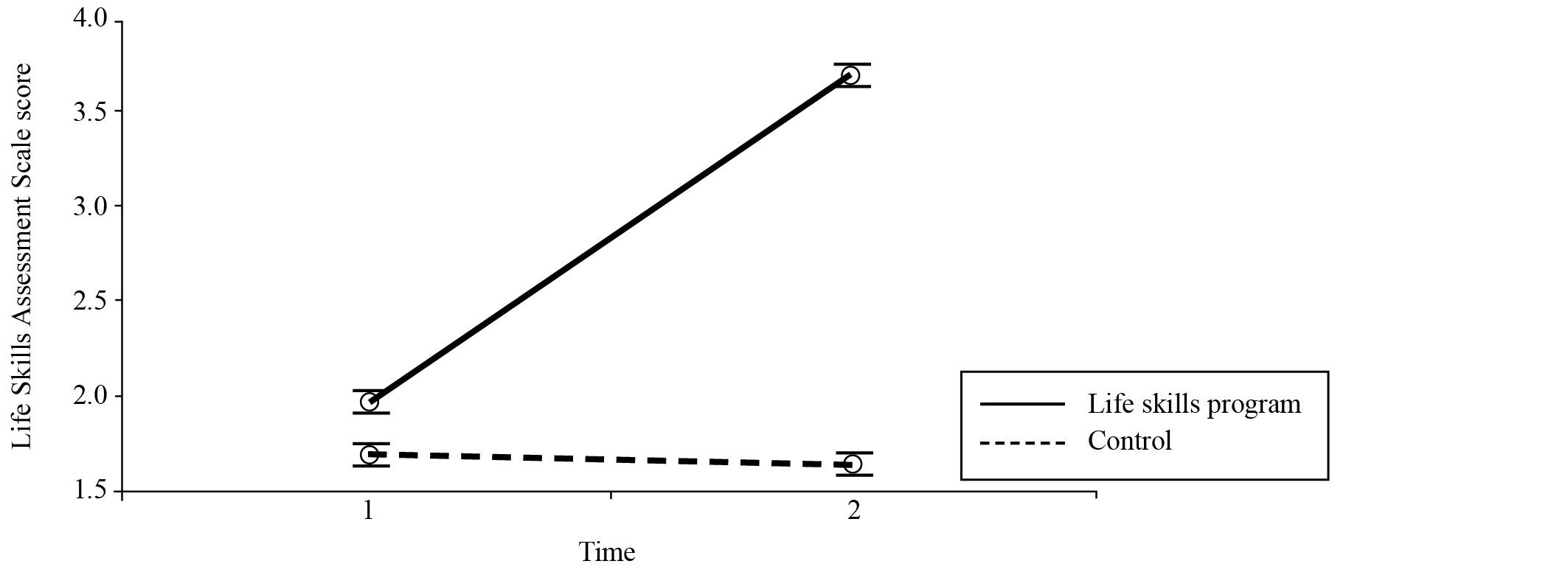
Figure 1. Mean Life Skills Assessment Scale Scores
Note. Time 1 = pregroup score; Time 2 = postgroup score. Error bars indicate 95% confidence intervals.
Discussion
The results in this study indicate that participation in an enrichment program for disadvantaged children (aged 8–15 years) in the developing world increased life skills with very large effects. As predicted, there was a significant increase in observer-rated life skills for those attending the enrichment program compared to the control group. These children, because of their socioeconomic status, are vulnerable to the cognitive, emotional, and social development delays associated with early adversity, and have minimal access to statutory services. Such delays can cause long-term if not lifelong deficits in the skills needed to function effectively in everyday life (Alderman et al., 2006; Brown & Pollitt, 1996; Pollitt et al., 1993; Victora et al., 2008). The results in our study indicate that low-budget programs using nonprofessionally trained facilitators can ameliorate such delays. Highly trained professionals and large budgets may not be required to attenuate the devastating effects of severe poverty and adversity that blight the development of millions of children.
Further research is needed to explore whether simple and scalable programs for children aged 5–15 years, and for young adults (cf. Pearson et al., 2021), positively affect participants’ wider developmental and mental health issues in the longer term. The structured enrichment program examined in this study had a considerable impact on the life skills of the children who took part. Longitudinal research is currently underway to establish whether these changes are maintained. It will also be important to determine if such programs need to impact on each stage of child development as the catching-up process gets underway. This raises the important question of whether these programs could kick-start aspects of delayed development, or if they simply increase life skills at any given point. The results in our study indicate that delays to cognitive, emotional, and social development as a result of adversity can be at least partly recoverable through simple, low-cost programs. Whether complete recovery is possible is yet to be established.
As our methodology was based on child development norms that are relevant cross-culturally, the results are likely to be generalizable to disadvantaged children across the countries and cultures of the developing world. Simple enrichment interventions based on sports and creative arts activities hold a cross-cultural and non-gender-specific appeal for children. The global pattern of severe adversity is changing rapidly, with increases in climate change, displaced children, refugees, war zones, and other emergencies and natural disasters. Simple structured programs could prove both effective in addressing the damage to children’s development typically seen in these situations, and cost effective as professionally trained staff, infrastructure, or even buildings are not necessarily required.
The key limitation of this study is that we did not have an active control group. This means that we cannot attribute the effects we found to the specific activities offered. Further research is required in which the program is compared with a control group offered at the same frequency and duration of contact. Additionally, assessments were completed during the initial and final sessions of the program rather than immediately before and after the program period, and the children were not necessarily assessed in the same order on these two occasions. Each of these issues could be addressed in future work. The study is also limited by the fact that the two groups differed in age, in that the children in the intervention group were slightly younger than those in the control group, and because the children in the intervention group had slightly higher LSAS scores at the start of the study than the control group. Nevertheless, the analyses show there were large improvements in observer-assessed life skills following the program. Other limitations relate to the study being run in real-world conditions with no dedicated funding. The allocation to group (program or control) was not random, and although we sought to ensure that participants and facilitators were unaware of the research details and group allocation, this could not be guaranteed. For these reasons the study was classed as a pragmatic randomized controlled trial (Dal-Ré et al., 2018), which arguably has greater generalizability in the field than does a standard randomized controlled trial (Salive, 2017).
Appendix: Life Skills Assessment Scale
Please complete this scale while observing, or as soon as possible after observing, the young person. You may need to spend some time observing before you decide. Do not spend too long thinking about each question, just record your impression. For each question, consider age appropriateness (think of actual age, rather than physical appearance).
Put a ✓ in one most relevant box for each question. The blank boxes can be used to note down things you saw that helped you fill in the boxes or for any other comments. You do not always have to fill in the comment boxes.
Alderman, H., Hoddinott, J., & Kinsey, B. (2006). Long term consequences of early childhood malnutrition. Oxford Economic Papers, 58(3), 450–474.
https://doi.org/10.1093/oep/gpl008
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Author.
https://doi.org/10.1176/appi.books.9780890425596
Benítez-Bribiesca, L., De la Rosa-Alvarez, I., & Mansilla-Olivares, A. (1999). Dendritic spine pathology in infants with severe protein-calorie malnutrition. Pediatrics, 104(2), Article e21.
https://doi.org/10.1542/peds.104.2.e21
Benoit, D., & Coolbear, J. (2003). Disorders of attachment and failure to thrive in attachment issues. In L. Atkinson & S. Goldberg (Eds.), Attachment issues in psychopathology and intervention (pp. 49–65). Erlbaum.
https://doi.org/10.4324/9781410609670
Birrell, R., Orley, J., Evans, V., Lee, J., Sprunger, B., & Pellaux, D. (1997). Life skills education for children and adolescents in schools. World Health Organization. https://bit.ly/2RIrvTI
Bloss, E., Wainaina, F., & Bailey, R. C. (2004). Prevalence and predictors of underweight, stunting, and wasting among children aged 5 and under in Western Kenya. Journal of Tropical Pediatrics, 50(5), 260–270.
https://doi.org/10.1093/tropej/50.5.260
Boddy, J., Skuse, D., & Andrews, B. (2000). The developmental sequelae of nonorganic failure to thrive. The Journal of Child Psychology and Psychiatry, 41(8), 1003–1014.
https://doi.org/10.1111/1469-7610.00688
Brown, J. L., & Pollitt, E. (1996). Malnutrition, poverty and intellectual development. Scientific American, 274(2), 38–43. https://bit.ly/3unrh1L
Ceylan, R., & Gök Çolac, F. (2019). The effect of drama on the life skills of five-year-old children. International Education Studies, 12(8), 46–58.
https://doi.org/10.5539/ies.v12n8p46
Cordero, M. E., d’Acuña, E., Benveniste, S., Prado, R., Nuñez, J. A., & Colombo, M. (1993). Dendritic development in neocortex of infants with early postnatal life undernutrition. Pediatric Neurology, 9(6), 457–464.
https://doi.org/10.1016/0887-8994(93)90025-8
Dal-Ré, R., Janiand, P., & Ioannidis, J. P. A. (2018). Real-world evidence: How pragmatic are randomized controlled trials labelled as pragmatic? BMC Medicine, 16, Article 49.
https://doi.org/10.1186/s12916-018-1038-2
Daniel, B., Wassell, S., & Gilligan, R. (2010). Child development for child care and protection workers (2nd ed.). Jessica Kingsley Publishers. https://bit.ly/3yBBjPR
De Bellis, M. D., Spratt, E. G., & Hooper, S. R. (2011). Neurodevelopmental biology associated with childhood sexual abuse. Journal of Child Sexual Abuse, 20(5), 548–587.
https://doi.org/10.1080/10538712.2011.607753
de Onis, M., & Branca, F. (2016). Childhood stunting: A global perspective. Maternal & Child Nutrition, 12(S1), 12–26.
https://doi.org/10.1111/mcn.12231
Drewett, R. F., Corbett, S. S., & Wright, C. M. (2005). Physical and emotional development, appetite and body image in adolescents who failed to thrive as infants. The Journal of Child Psychology and Psychiatry, 47(5), 524–531.
https://doi.org/10.1111/j.1469-7610.2005.01529.x
Dykman, R. A., Casey, P. H., Ackerman, P. T., & McPherson, W. B. (2001). Behavioral and cognitive status in school-aged children with a history of failure to thrive during early childhood. Clinical Pediatrics, 40(2), 63–70.
https://doi.org/10.1177/000992280104000201
Essex, M. J., Klein, M. H., Cho, E., & Kalin, N. H. (2002). Maternal stress beginning in infancy may sensitize children to later stress exposure: Effects on cortisol and behaviour. Biological Psychiatry, 52(8), 776–784.
https://doi.org/10.1016/S0006-3223(02)01553-6
Grantham-McGregor, S., Cheung, Y. B., Cueto, S., Glewwe, P., Richter, L., Strupp, B., … The International Child Development Steering Group. (2007). Developmental potential in the first 5 years for children in developing countries. Lancet, 369(9555), 60–70.
https://doi.org/10.1016/S0140-6736(07)60032-4
Hoddinott, J., Behrman, J. R., Maluccio J. A., Melgar, P., Quisumbing, A. R., Ramirez-Zea, M., … Martorell, R. (2013). Adult consequences of growth failure in early childhood. The American Journal of Clinical Nutrition, 98(5), 1170–1178.
https://doi.org/10.3945/ajcn.113.064584
Jaffe, A. C. (2011). Failure to thrive: Current clinical concepts. Pediatrics in Review, 32(3), 100–108.
https://doi.org/10.1542/pir.32-3-100
Kennedy, F., Kennerley, H., & Pearson, D. (Eds). (2013). Cognitive behavioural approaches to the understanding and treatment of dissociation. Routledge.
https://doi.org/10.4324/9780203502082
Kennedy, F., Pearson, D., Brett-Taylor, L., & Talreja, V. (2014). The Life Skills Assessment Scale: Measuring the life skills of disadvantaged children in the developing world. Social Behavior and Personality: An international journal, 42(2), 197–209.
https://doi.org/10.2224/sbp.2014.42.2.197
Kessler, R. C., McLaughlin, K. A., Green, J. G., Gruber, M. J., Sampson, N. A., Zaslavsky, A. M., … Williams D. R. (2010). Childhood adversities and adult psychopathology in the WHO World Mental Health Surveys. The British Journal of Psychiatry, 197(5), 378–385.
https://doi.org/10.1192/bjp.bp.110.080499
Kinderman, P., Schwannauer, M., Pontin, E., & Tai, S. (2013). Psychological processes mediate the impact of familial risk, social circumstances and life events on mental health. PLOS ONE, 8(10), Article 76564.
https://doi.org/10.1371/journal.pone.0076564
Korzekwa, M. I., Dell, P. F., & Pain, C. (2009). Dissociation and borderline personality disorder: An update for clinicians. Current Psychiatry Reports, 11, 82–88.
https://doi.org/10.1007/s11920-009-0013-1
Larson-Nath, C., & Biank, V. F. (2016). Clinical review of failure to thrive in pediatric patients. Pediatric Annals, 45(2), e46–e49.
https://doi.org/10.3928/00904481-20160114-01
Mackner, L. M., Starr, R. H., Jr., & Black, M. M. (1997). The cumulative effect of neglect and failure to thrive on cognitive functioning. Child Abuse & Neglect, 21(7), 691–700.
https://doi.org/10.1016/S0145-2134(97)00029-X
Mahapatra, D. (2014, February 23). India witnessing NGO boom: There is 1 for every 600 people. The Times of India. https://bit.ly/347M26G
Mandigo, J., Corlett, J., Holt, N., van Ingen, C., Geisler, G., MacDonald, D., & Higgs, C. (2018). The impact of the Hoodlinks Programme on developing life skills and parenting youth violence in Guatemala City. Journal of Sport for Development, 6(11), 21–37. https://bit.ly/3oKJmpi
Mendelsohn, R., Dinar A., & Williams L. (2006). The distributional impact of climate change on rich and poor countries. Environment and Development Economics, 11(2), 159–178.
https://doi.org/10.1017/S1355770X05002755
Mendez, M. A., & Adair, L. S. (1999). Severity and timing of stunting in the first two years of life affect performance on cognitive tests in late childhood. The Journal of Nutrition, 129(8), 1555–1562.
https://doi.org/10.1093/jn/129.8.1555
Ministry of Statistics and Programme Implementation, Government of India. (2012). Children in India 2012 - A statistical appraisal. Author. https://bit.ly/3wqXQNw
Naandi Foundation. (2012). HUNGaMA: Fighting hunger and malnutrition: The HUNGaMA Survey Report – 2011. Author. https://bit.ly/2QKBYgZ
Olinto, P., Beegle, K., Sobrado, C., & Uematsu, H. (2013). The state of the poor: Where are the poor, where is extreme poverty harder to end, and what is the current profile of the world’s poor? Economic Premise, 125, 1–8. https://bit.ly/3fAPsnQ
Pearson, D. (2013). Can the roots of dissociation be found in childhood? In F. Kennedy, H. Kennerley, & D. Pearson (Eds.), Cognitive behavioural approaches to the understanding and treatment of dissociation (pp. 40–52). Routledge.
https://doi.org/10.4324/9780203502082
Pearson, D., Kennedy, F., Talreja, V., Bhat, S., & Newman-Taylor, K. (2020). The Life Skills Assessment Scale: Norms for young people aged 17–19 and 20–22 years. Social Behavior and Personality: An international journal, 48(4), e8938.
https://doi.org/10.2224/sbp.8938
Pearson, D., Kennedy, F., Talreja, V., Bhat, S., & Newman-Taylor, K. (2021). Thriving in adversity: Do brief milieu interventions work for developing world young adults? A pragmatic randomized controlled trial. Social Behavior and Personality: An international journal, 49(9), e10494.
https://doi.org/10.2224/sbp.10494
Pollitt, E., Gorman, K. S., Engle, P. L., Martorell, R., Rivera, J., Wachs, T. D., & Scrimshaw, N. S. (1993). Early supplementary feeding and cognition: Effects over two decades. Monographs of the Society for Research in Child Development, 58(7), 115–118.
https://doi.org/10.2307/1166162
Read, J., & Bentall, R. P. (2012). Negative childhood experiences and mental health: Theoretical, clinical and primary prevention implications. The British Journal of Psychiatry, 200(2), 89–91.
https://doi.org/10.1192/bjp.bp.111.096727
Salive, M. (2017, June 7). Pragmatic clinical trials: Testing treatments in the real world. National Institute of Aging. https://bit.ly/3wmVW0i
Save the Children’s Resource Centre. (2017). Stolen childhoods: End of childhood report 2017. Author. https://bit.ly/3hOlWxO
Sawhill, J., & Williamson, D. (2001, May 1). Measuring what matters in nonprofits. The McKinsey Quarterly, 2, 98–107. https://mck.co/3oPCA1l
United Nations International Children’s Emergency Fund. (2009). The state of the world’s children. Author. https://uni.cf/3ucu2Tq
United Nations International Children’s Emergency Fund. (2016, October 3). Nearly 385 million children living in poverty says joint World Bank Group-UNICEF study. Author. https://uni.cf/3hKkyMB
United Nations International Children’s Emergency Fund, World Health Organization, and The World Bank Group. (2017). Joint child malnutrition estimates – Levels and trends in child malnutrition (2017 edition). World Health Organization.
Van der Vegt, E. J. M., van der Ende, J., Huizink, A. C., Verhulst, F. C., & Tiemeier, H. (2010). Childhood adversity modifies the relationship between anxiety disorders and cortisol secretion. Biological Psychiatry, 68(11), 1048–1054.
https://doi.org/10.1016/j.biopsych.2010.07.027
Victora, C. G., Adair, L., Fall, C., Hallal, P. C., Martorell, R., Richter, L., & Sachdev, H. S. (2008). Maternal and child undernutrition: Consequences for adult health and human capital. The Lancet, 371(9609), 340–357. https://bit.ly/3bQZH6y
Woldehanna, T., Behrman, J. R., & Araya, M. W. (2017). The effect of early childhood stunting on children’s cognitive achievements: Evidence from Young Lives Ethiopia. Ethiopian Journal of Health Development, 31(2), 75–84. https://bit.ly/3hNm8gB
World Bank Group. (2018). Poverty and shared prosperity 2018: Piecing together the poverty puzzle. Author. https://bit.ly/3febqxV
Table 1. Psychological Effects of Severe Childhood Adversity and Failure to Thrive
Note. Adapted from Pearson et al. (2020).
Table 2. Gender and Age of Participants by Group
Table 3. Descriptive Statistics for the Life Skills Assessment Scale Scores
Figure 1. Mean Life Skills Assessment Scale Scores
Note. Time 1 = pregroup score; Time 2 = postgroup score. Error bars indicate 95% confidence intervals.
This research received no specific grant from any funding agency
commercial
or not-for-profit sectors.
The authors acknowledge the tireless contributions made by Khushboo Kumari
Annie Jacob
Sheetal Lydia Prasad
and Chandrasekhar for this study.
David Pearson, The Boulders, Quarr Road, Ryde, IoW, PO33 4EL, United Kingdom. Email: [email protected]