The effectiveness of a web-based positive psychology intervention in enhancing college students’ mental well-being
Main Article Content
During the global pandemic, lockdown policies aimed at curbing the spread of COVID-19 have been affecting all demographics. Although they may be continuing their studies online, university students may suffer severe mental consequences because of loneliness and social isolation. To help students improve their psychological well-being, we examined the effectiveness of a web-based positive psychology intervention (PPI) with 886 students who either took part in PPI sessions or received health reminders. Results show that the PPI sessions (vs. regular health reminders) significantly improved positive mood and mitigated negative emotions among the students. The positive effect of the intervention also remained consistent at both 3- and 6-month follow-ups. These findings indicate that PPI should be embraced at universities to boost college students’ psychological state.
The outbreak of the coronavirus disease 2019 (COVID-19) has caused unprecedented destruction of economic, medical, and educational systems along with a human death toll of more than 1.99 million worldwide, as of January 15, 2021 (World Health Organization, n.d.). With the aim of curtailing human transmission, governments in most countries have initiated lockdown policies. Consequently, to protect students from possible infection, at many universities in-classroom teaching has been suspended (Bowen, 2020) in favor of remote learning via online courses. In addition, millions of college students have been notified that a return date to normal campus life cannot be confirmed until the pandemic is significantly controllable.
However, it should be noted that self-isolation and school closures may result in severe psychological consequences for students, who are often prone to compounding negative emotions when schools are closed regularly for vacations (Van Bortel et al., 2016). N. Liu et al (2020) found that 7% of college students in one of the areas of China hit hardest by the COVID-19 pandemic have manifested symptoms of posttraumatic stress, including negative intrusive thoughts, being immersed in traumatic memory, emotional numbing, and physiological hyperarousal. The pandemic has resulted in a collective panic permeating the entire Chinese university student community (Wang & Zhao, 2020). Clearly, to avert the deterioration of mental health conditions induced by the COVID-19 pandemic and halt their increase, students require effective psychological interventions. Hence, to avoid negative ramifications for the mental health of students, it is essential that those responsible for student well-being respond to this situation quickly and appropriately.
Given that traditional face-to-face counselling therapy is not possible under the confines of social distancing policies (Walsh et al., 2006), feasible positive psychology interventions (PPI) are scarce. In addition, the main focus of traditional mental health support services, including talking therapy and other similar treatments, is on tackling negative or difficult past experiences (Jaberghaderi et al., 2004). Without undermining the importance of recognizing and comprehending the psychological pain of the individual through therapeutic sessions, it should be mentioned that patients periodically report feeling “stuck in a loop of negative thinking” when therapists continually attempt to evoke past unpleasant memories (Conoley et al., 2015). It is, thus, possible that students suffering with pandemic-related mental difficulties may experience increased confusion if, via remote channels and without the physical presence of professional instructions provided by a therapist, they were to be exposed to unfamiliar contexts of conventional psychological treatment. To avoid impeding improvement of mental health, an innovative approach must be developed and applied that transcends the framework of traditional psychological therapy. Considering the mental distress features resulting from the ongoing coronavirus crisis, PPI, a new subcategory of the psychological sciences, in which the emphasis is on eliciting positive emotions, could be recommended as a valid approach for treating collegiate mental health problems.
The objective in PPI is to teach people methods of initiating positive emotions that lead to a eudemonic life (Seligman, 2012). In these interventions the focal point is not only changed from negative experiences to pleasant moments, but meaningful activities beneficial to developing an individual’s potential are also promoted by providing that person with self-help guidance (Diener et al., 1999). The compatibility and efficacy of PPI in coping with persistent stress has the advantages of encouraging self-awareness and eliciting positive empathy (Antoine et al., 2018). Seligman et al. (2006) found that positive psychotherapy exercises administered on a web-based platform significantly relieved depressive symptoms among university students for at least 6 months, compared with a control group receiving placebo interventions.
In the battle against the negative mental health consequences that the global pandemic is inflicting on society, and based on the merits of PPI, it is crucial that a positive psychology perspective is brought to public awareness. However, the psychological consequences of this pandemic are still a recent development, and the literature is scant regarding the effects of PPI programs on the psychological well-being of university populations in the era of social distancing and remote learning. In addition, few web-based PPI programs have to date been translated into languages other than English, or adjusted with respect to cultural background. Therefore, studies are urgently required to explore whether a web-based PPI program could serve as an efficacious intervention for alleviating the mental distress of college students during the COVID-19 pandemic, and also to offer an optimistic outlook for the future.
We analyzed the literature on PPI techniques and aimed to examine, for the first time, the general effectiveness of delivering PPI online to university students in China for improving their mental well-being during the lockdown period of the COVID-19 pandemic. Thus, we proposed the following hypothesis:Compared to those receiving only regular health well-being reminders via email, the positive mood of university students receiving a web-based positive psychology intervention program will be enhanced and their negative emotions will be relieved, both immediately and after a period of 3 to 6 months.
The independent variables in this study were the type of intervention (web-based PPI and health reminders) and assessment time points (baseline, posttreatment, after 3 months, and after 6 months). The dependent variables were students’ positive affect (PA) and negative affect (NA) scores.
Method
Participants
We initially recruited 1,000 second-year undergraduate students (500 women, 500 men) at Harbin University of Science and Technology, China, who were enrolled in the health psychology program run by the undergraduate administration division of the university. The data of 132 participants were removed because they did not submit complete responses. Thus, 868 students remained: 420 students in the PPI group and 448 in the control group. All participants were recruited from either the School of Computer Science and Technology or the School of Foreign Languages, with an age range of between 19 and 22 years (M = 20.40, SD = 0.53). The low dropout rate was within our expectation because participation in psychological activities contributes vital academic credits to students’ coursework.
Procedure
After obtaining approval from the Chinese Association for Ethical Studies in February 2020, we sent the participants an email containing a link to the consent form, demographic characteristics, and affective state measurements (https://bit.ly/3d3meh3) that have been specifically designed for undergraduate students in China. The demographic characteristics measure covered gender and age information, and their baseline affective state was evaluated with the short form of the Positive and Negative Affect Schedule (PANAS; Mackinnon et al., 1999). To ensure that every item in the PANAS was understood by the participants, we enlisted the help of professors at the School of Foreign Languages at Harbin University of Science and Technology to interpret and define each word using an accurate Chinese equivalent. To monitor the sustainability of maintaining the students’ optimism after completing the PPI, we also sent the PANAS again via email to all participants for reassessment at both 3- and 6-month follow-up time points.
All students who completed the consent form along with submitting baseline measurements were then randomly assigned to either the web-based PPI condition or the control condition. For those assigned to the PPI group, the web-based intervention program that followed positive psychological guidelines was sent to the respondent’s university email account. In accordance with the positive psychology treatment developed by Seligman and Csikszentmihalyi (2000), the web-based PPI incorporated two psychotherapeutic techniques: positive future imagination and gratitude-inducing thinking. The guidelines for these two techniques were translated into Chinese by two professors in English literature from the School of Foreign Languages at Harbin University of Science and Technology. Once participants had accessed the intervention website, which was also affiliated with Harbin University of Science and Technology, the instructions for positive future imagination based on the original version proposed by Sheldon and Lyubomirsky (2006) appeared on the screen. The step-by-step guide shown on the webpage was as follows:
- The exercise entails spending 1 minute thinking about the most exciting expectation for your upcoming campus life after our nation defeats coronavirus, and then writing down your thoughts. “Think about the most exciting expectation” means that you imagine your university life in the future, after the COVID-19 epidemic has tapered off thoroughly, when the normal routine of all universities will resume. You might achieve the greatest score in your department thanks to your hardworking mentality, win a basketball championship for your school, or even start a romantic relationship with your crush who is sitting next to you…
After reading the instructions, participants were asked to spend 15 minutes writing about their expected outcomes from their prospective university life. When they completed that task, the following instructions were given for the imagination part:
- Now that the 15-minute time for writing is over, bring to life as vividly as possible the things you have written by utilizing your imagination. Take 5 minutes to contemplate your life as your best possible self. Imagine your ideal future life at our university in as much detail as you can. Please make a mental note of the present feelings induced by your imagination regarding your future life expectation at our campus. You do not have to consciously retain these feelings, but if the feelings persist, you can relish and enjoy this psychological state until it gradually fades.
Participants who finished this step were able to proceed to the next PPI session by clicking the “Done” button on the bottom left of the page. Consequently, another email with the website link for the second session would automatically be generated. However, participants were required to complete the second session within 3 days of receiving the email in order to receive the postintervention assessment. The instructions for the second session of the PPI, which focused on gratitude-inducing thinking, were as follows:
- Although we are currently facing an unprecedented medical crisis, there are still many positive things going on in our lives for which we might be grateful. Please contemplate these feelings of gratitude that you have had even during the past weeks since we were told to be self-quarantined at home, and write down up to five things for which you are grateful or thankful during our recent isolation experience.
Immediately after completing the second session of PPI, participants received an automatically generated email directing them to return to the posttreatment assessment website. Follow-up assessments were successively sent to via email using the same format after 3 months and again after 6 months. However, participants could not access the follow-up test unless the previous assessment was successfully submitted online.
After the participants assigned to the control group had submitted the baseline measures, they received only mental health reminders sent to their university email account. The reminders contained regular informative content about health, including daily tips such as “wash your hands,” “wear a mask when going out,” and “stay optimistic about your life.” These reminders were sent to the control group members four times during the two weeks following their submission of the baseline measure, preceding their first postintervention assessment using the PANAS. The protocols for updating their follow-up psychological state after 3 and 6 months were identical to those for participants in the PPI group. To elucidate the timeline of intervention and control conditions, we compiled a timeline chart to depict the whole process (see Figure 1).
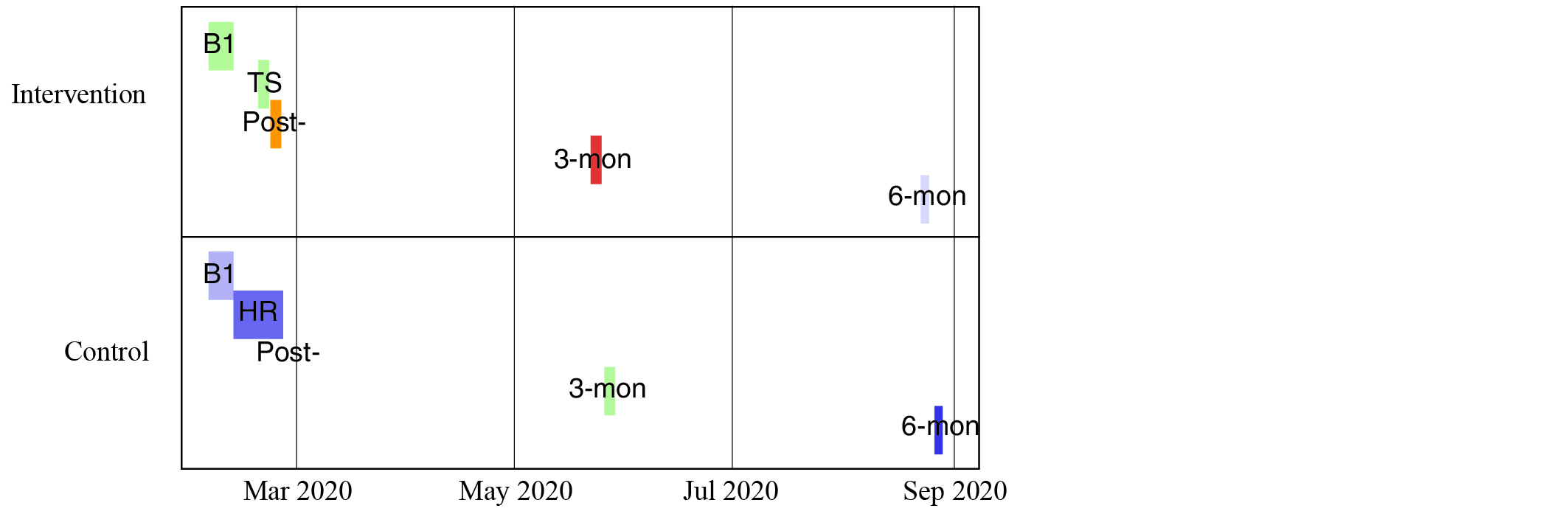
Figure 1. Experimental Timeline for Both Groups
Note. B1 = baseline measurement; TS = treatment sessions for PPI group; HR = health reminders for control group; Post = posttreatment assessment; 3-mon = follow-up assessment after 3 months; 6-mon = follow-up assessment after 6 months.
Upon completion of the last follow-up assessment, all participants could scan the QR code at the end of the assessment webpage to access the debriefing form.
Measures
We employed the abbreviated form of the PANAS (Mackinnon et al., 1999) to assess the general affective state of all participants. The PANAS is designed around 10 items of affect (five for PA, the other for NA) and comprises words that describe different emotions and feelings. Participants are instructed to read each item and use a 5-point Likert scale to indicate to what extent they feel these emotions at the moment: 1 (very slightly or not at all), 2 (a little), 3 (moderately), 4 (quite a bit), and 5 (extremely). The frame of reference was the current psychological state of the participant. This abbreviated PANAS was completed four times by all participants, at four time points (baseline, posttreatment, 3-month follow-up, and 6-month follow-up) amid the whole study period. Cronbach’s alphas indicating degree of internal consistency in this sample were .71, .75, .73 and .81 for the NA items and .73, .78, .72, and .79 for the PA items at the baseline assessment, postintervention evaluation, 3-month follow-up, and 6-month follow-up time points, respectively. These results are indicative of good internal consistency.
Data Analysis
R software and SPSS version 25 were used to compose the experimental timeline and to perform data analysis, respectively. Two 2 × 4 mixed-design analyses of variance (ANOVAs) with Bonferroni adjustments were applied to test the effectiveness of the PPI over the 6-month duration of the experiment.
Results
Baseline Characteristics and Affective State
Pearson’s chi-square test was performed to examine whether the distribution of genders differed across the PPI and control groups. Results show that the gender distribution was not significantly different across the two conditions, χ2(1,868) = .286, p = .593, V = .036. Table 1 shows the baseline characteristics for both groups, including gender and age, and baseline affective state as measured by the PANAS score. In addition, we ran two independent-samples t tests to assess whether there was a difference in PA and NA scores between the two groups in the pretest phase. Analyses revealed that neither PA nor NA scores differed significantly for the two groups (see Table 1).
Table 1. Baseline Characteristics and Affective State of Participants
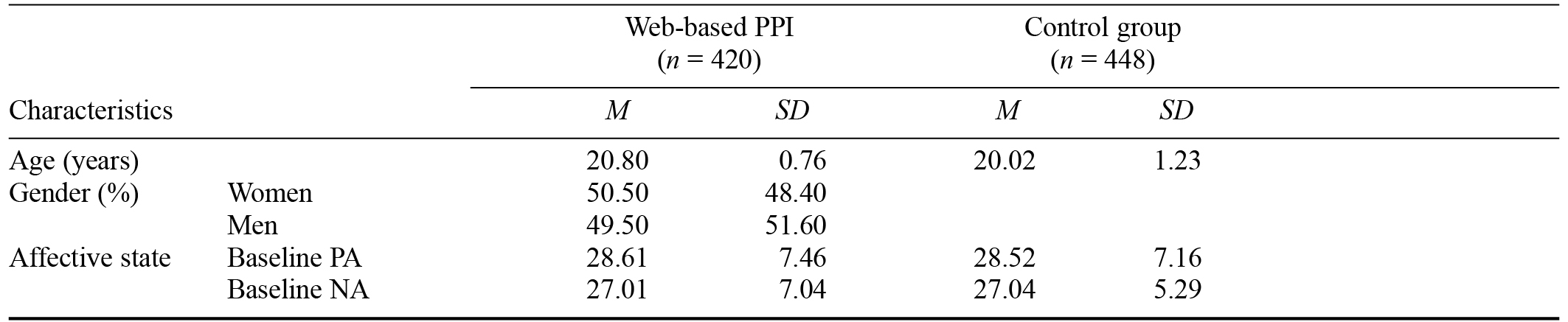
Note. PPI = positive psychology intervention; PA = positive affect score; NA = negative affect score.
Assessment of Effectiveness of the Positive Psychology Intervention Program at Each Phase of Treatment
Positive Affect
We used a 2 (condition: intervention vs. control) × 4 (time: baseline vs. posttreatment vs. 3-month follow-up vs. 6-month follow-up) mixed model ANOVA with the treatment type as the between-subjects variable and each time point of assessment as the within-subjects variable to test the PA of the students. There was a significant main effect of type of treatment, F(1, 866) = 172.88, p < .001, ηp2 = .166, a significant main effect of different phases of assessment, F(3, 2598) = 52.07, p < .001, ηp2 = .057, and a significant interaction between type of treatment and the time point of assessment, F(3, 2598) = 20.51, p < .001, ηp2 =.023, on the outcome of PA. The main effect of treatment type reveals that participants who received the web-based PPI scored higher on PA (M = 31.73, SE = 0.17) than did participants who received only regular health notifications and reminders (M = 28.54, SE = 0.17). The main effect of time point demonstrates that students’ PA score was still significantly different at certain phases, regardless of their randomized condition.
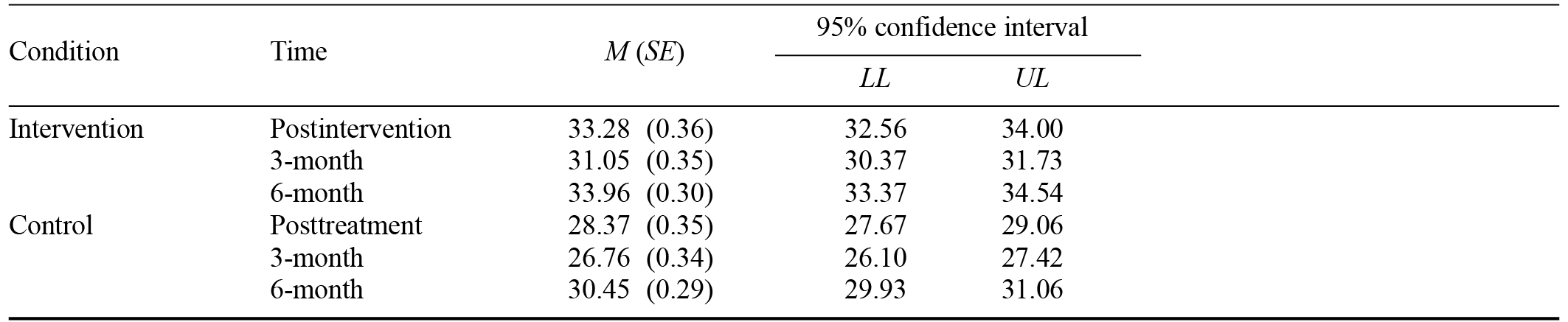
Regarding the interaction effect, among participants at the posttreatment, 3-month follow-up, and 6-month follow-up time points, those undertaking the PPI sessions scored significantly higher (p < .01) on PA (M = 33.28, SE = 0.36; M = 31.05, SE = 0.35; M = 22.96, SE = 0.30) than did those who received only health reminders (M = 28.37, SE = 0.35; M = 26.76, SE = 0.34; M = 30.50, SE = 0.29). Furthermore, participants assigned to the PPI group gained 4.66, 2.44, and 5.34 more PA points at the posttreatment phase, 3-month follow-up, and 6-month follow-up, respectively, compared to the baseline PA score (p < .001). In addition, the PA score for the PPI group was 2.90 points higher at the 6-month follow-up than that measured at the 3-month follow-up (p < .001). However, the PA scores at the 6-month and 3-month follow-ups were nonsignificantly different from those at the posttreatment assessment, p = .14. Among all the students in the control group, the PA score was nonsignificantly different at posttreatment compared to the baseline assessment (p = .76). Furthermore, the PA score at the 3-month follow-up was 1.77 points lower than that at baseline and 1.61 points lower than that at posttreatment (p < .001). In contrast, the PA score obtained at the 6-month follow-up was significantly improved by 1.97 points compared with baseline, 2.13 points compared with posttreatment, and 3.74 points compared with the 3-month follow-up phase (p < .001). The outcomes of main and interaction effects on PA scores are summarized in Table 2.
Table 2. Summary of Interaction Effects and 95% Confidence Intervals for Positive Affect Scores According to Condition
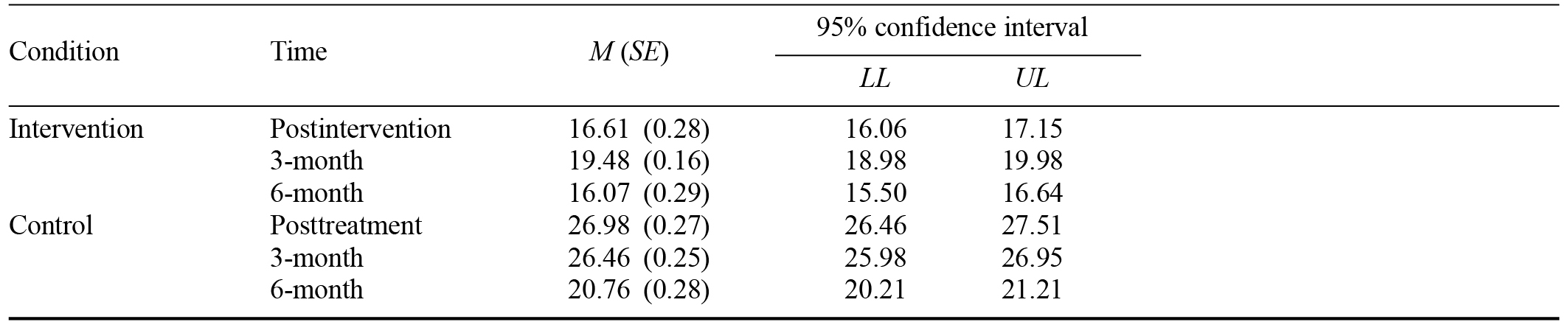
Note. LL = lower limit; UL = upper limit.
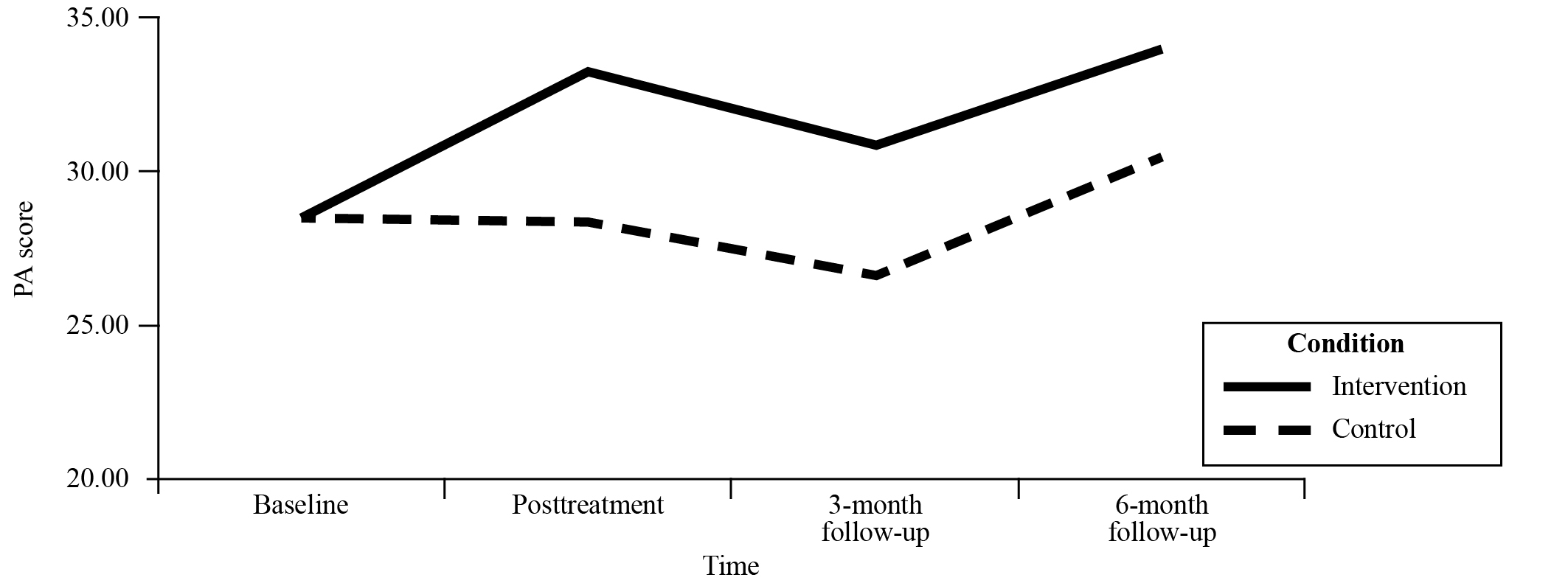
Figure 2. Positive Affect Score in Both Groups
Note. PA = positive affect.
Negative Affect
We used another 2 (condition: intervention vs. control) × 4 (time: pretest vs. posttreatment vs. 3-month follow-up vs. 6-month follow-up) mixed-model ANOVA with treatment type as the between-subjects variable and follow-up time point as the within-subjects variable to examine participants’ NA. There was a significant main effect of type of treatment, F(1, 866) = 817.18, p < .001, ηp2 = .485, a significant main effect of the length of time before follow-up, F(3, 2598) = 326.81, p < .001, ηp2 = .274, and a significant interaction between type of treatment and follow-up time point, F(3, 2598) = 122.15, p < .001, partial ηp2 = .124, on the outcome of NA. The main effect of treatment type shows that participants who received the web-based PPI scored lower on NA (M = 19.79, SE = 0.14) than did participants who received only regular psychological well-being reminders or notifications (M = 25.31, SE = 0.13). The main effect of the follow-up time demonstrates that if the factors of condition difference were ruled out, participants scored fewer NA points at the 6-month follow-up (M = 18.42, SE = 0.20) than they did at baseline, posttreatment, and the 3-month follow-up (M = 27.02, SE = 0.21; M = 21.79, SE = 0.19; M = 22.97, SE = 0.18), respectively. However, the NA score was significantly (p < .001) higher at the 3-month follow-up time point in comparison with the other three time points. Figure 3 illustrates how the NA score changed over the 6 months of the experiment.
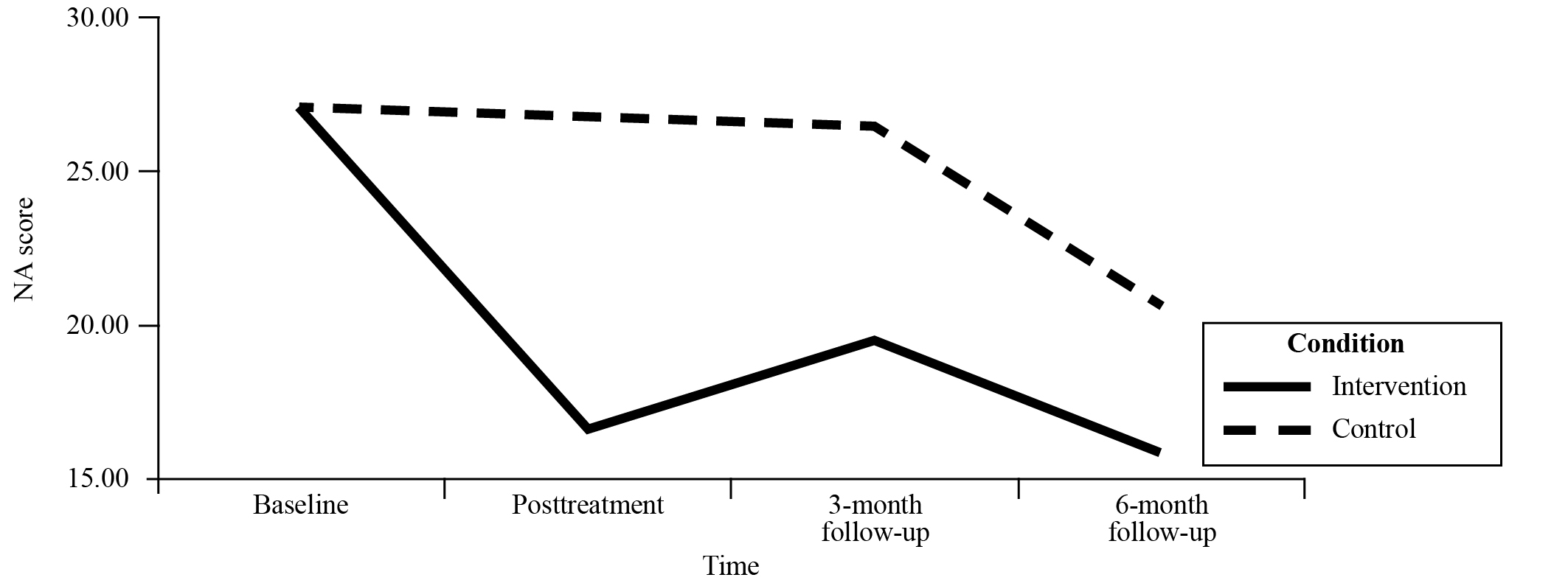
Figure 3. Negative Affect Score in Both Groups
Note. NA = negative affect.
With respect to the interaction effect, the NA scores of the PPI group were 10.38 points lower at posttreatment, 6.98 points lower at 3-month follow-up, and 4.69 points lower at 6-month follow-up compared to the scores of those in the control group (ps < .001). In addition, among those assigned to the PPI condition, the NA score significantly declined at posttreatment, 3-month follow-up, and 6-month follow-up time points compared to their scores at baseline by 10.41, 7.54, and 10.95 points, respectively. The difference in NA scores between posttreatment and 3-month follow-up, however, was not significant (p = .19). In addition, the NA score showed more negative affect by 2.87 at the 3-month time point compared to that at posttreatment (p < .001). For the control group, the only significant decrease of NA score was observed at the 6-month time point. The score at that time was 6.38 lower than at baseline, 6.22 points lower than at posttreatment, and 5.70 points lower compared to at the 3-month assessment (p < .001). In contrast, the NA score at posttreatment had not changed significantly with reference to baseline assessment (p = .89). Additionally, the NA score at the 3-month follow-up had not altered significantly compared to both baseline assessment (p = .14) and posttreatment (p = .14). The NA scores defined by main and interaction effects of these two factors are shown in Tables 3 and 4.
Table 3. Means and Standard Deviations for the Main Effects of Positive and Negative Affect According to Condition
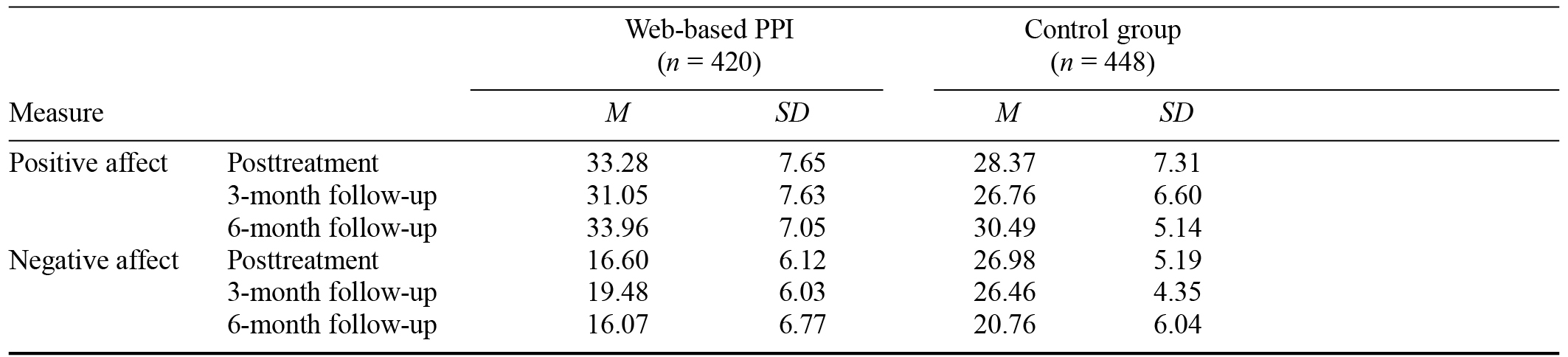
Note. PPI = positive psychology intervention.
Table 4. Summary of Interaction Effects and 95% Confidence Intervals for Negative Affect Score According to Condition
Note. LL = lower limit; UL = upper limit.
Discussion
Restrictive stay-at-home policies during the COVID-19 pandemic have affected all demographics, including university students who, although continuing with their curriculum online, may suffer severe mental consequences because of loneliness and social isolation. In this study we confirmed that a web-based PPI program can significantly increase PA while attenuating NA among university students. This is consistent with previous research demonstrating that imagining positive events can play a pivotal role in the underlying procedure of cognitive bias modification (Holmes et al., 2009). In addition, this implies that the psychological well-being of students living in circumstances where face-to-face communication with their classmates and/or teachers is limited can be improved when the students are provided with an appropriate PPI program. However, producing an intervention appropriate for a unique demographic requires complex amendments of the intervention to suit the milieu. One of the difficulties we faced in this study was the lack of Chinese literature guiding composition of a PPI program. To adapt to the context of Chinese universities, we collaborated with two senior professors teaching at the School of Foreign Languages at Harbin University of Science and Technology. With their assistance, we interpreted the original version of positive intervention techniques, including positive future imagination and gratitude-inducing thinking (Seligman & Csikszentmihalyi, 2000) into contemporary Chinese language comprehensible to young Chinese people born after 2000.
Regarding the hypothesis, not only did we find that the PPI group scored significantly higher on PA and significantly lower on NA when compared to the control group at all assessment phases, but we were also surprised to note the result that for both groups the NA score was significantly lowered at the 6-month follow-up when compared with those at baseline assessment and at the 3-month follow-up assessment. This finding corroborates those of previous studies in which it has been asserted that a web-based PPI program can help relieve depressive symptoms for at least 6 months after the last intervention session (Seligman et al., 2006). However, this result may imply only that the Chinese version of the web-based PPI has a better prognosis even at a longer follow-up time point, which appears to contradict clinical commonsense that the effectiveness of a treatment is always somewhat diminished after time (Kennard et al., 2009). However, we attribute this, in part, to the successful control of COVID-19 by the Chinese government, as businesses and schools resumed their normal mode of functioning by August 2020, with most students required to return to universities where in-class activities were permitted with students wearing face masks and observing appropriate social distancing. It can, therefore, be assumed that as the new semester approached and all students could return to their university, there would be an accompanying sense of relief and even exhilaration.
Furthermore, the longevity of the effectiveness of PPI found in our study also complies with the unique advances of the positive psychology approach, that is, the broaden-and-build theory of positive emotions (Fredrickson & Joiner, 2002). Fredrickson and Joiner (2002) described how gaining emotions with positive valence boosts the likelihood of inducing more positive emotions in the future, which generally equates to upward motion toward well-being. Thus, PPI has a long-lasting outcome when combating enduring stress. In a study that included students from 48 universities, Marrero et al. (2016) found that cognitive behavioral therapy combined with PPI significantly augmented students’ subjective and eudemonic well-being. Hence, because of the long-term effectiveness of PPI, the discovery of its capacity to combine with other psychological treatments and to be shared via online interventions offers great hope to those in the field of psychology.
Finally, we conducted our study with a large sample of 868 participants, who completed each phase of testing from baseline screening to 6-month follow-up. Another merit of this study is the best fit representation of Chinese university students, in that all participants were second-year undergraduate students. This is considered the best fit representation because the curriculum for first-year Chinese university students is designated an academic transition between high school and college, and third-year students mostly concentrate on off-campus internships, suggesting that only second-year undergraduate Chinese students focus their full attention on their university curriculum and activities. Moreover, our sampling strategy substantially eliminated possible gender bias in the distribution of the sample. As the participants recruited in this study were all from the School of Computer Science and Technology or the School of Foreign Languages, where gender ratios of males to females are 9 to 1 and 1 to 9, respectively, we are confident that a sample of students from these two schools could be mutually complementary in terms of equilibrium of gender distribution, even under a randomized method of assigning participants to the PPI or control groups. As a result, the proportion of men to women for this study almost reached 50/50.
Limitations and Future Research Directions
Our study has several limitations offering opportunities for further study. First, we lacked certain demographic information; for example, socioeconomic status was not included in the baseline characteristics, as asking for a student’s family annual income or parents’ occupation from departments other than the Ministry of Admission would be considered a possible violation of a student’s self-esteem. However, a person’s socioeconomic status could be an underlying factor in their general well-being (Watson et al., 1999). Another limitation is that the measure we used was not designed for medical conditions, such as clinically diagnosed depression or anxiety disorder; thus, whether there was a significant effect of the web-based PPI on the relief of symptoms of mental illness remains unknown. This suggests that further research, such as randomized controlled trials, should be implemented soon. Finally, although we tried to manipulate an identical timeline in both conditions, there was still approximately a 5- to 7-day difference between the PPI group and the control group in terms of allocating treatment and receiving feedback at each treatment or assessment stage over the course of the 6-month duration of the experiment. This time difference may have resulted in risks of exacerbating psychological stress in either group because of delay in being treated with the designated intervention.
Conclusion
In sum, our study findings support the use of web-based PPI precluding disastrous mental health consequences for most university students not allowed to return to the classroom during this pandemic. Considering that COVID-19 is an ongoing crisis that will possibly last a considerable time, the imminent focus should not only include an effective vaccination program against this coronavirus disease, but also a “cognitive vaccine” (Holmes et al., 2009) for treating the psychological stresses related to the pandemic and self-isolation. As researchers in this dark period in human history, we feel that helping societies return to normalcy may be the underlying factor for exponentially reducing stress. This requires an efficient, all-inclusive public health policy with reference to curbing the transmission of coronaviruses. As such, we urge the world’s governments to temporarily set aside political disputes to engage in an international collaboration of health and welfare protection.
References
Antoine, P., Dauvier, B., Andreotti, E., & Congard, A. (2018). Individual differences in the effects of a positive psychology intervention: Applied psychology. Personality and Individual Differences, 122, 140–147.
https://doi.org/10.1016/j.paid.2017.10.024
Bowen, M. (2020). COVID-19 has changed how we teach students. The Veterinary Record, 186(14), 461.
https://doi.org/10.1136/vr.m1535
Conoley, C. W., Pontrelli, M. E., Oromendia, M. F., Del Carmen Bello, B., & Nagata, C. M. (2015). Positive empathy: A therapeutic skill inspired by positive psychology. Journal of Clinical Psychology, 71(6), 575–583.
https://doi.org/10.1002/jclp.22175
Diener, E., Suh, E. M., Lucas, R. E., & Smith, H. L. (1999). Subjective well-being: Three decades of progress. Psychological Bulletin, 125(2), 276–302.
https://doi.org/10.1037/0033-2909.125.2.276
Fredrickson, B. L., & Joiner, T. (2002). Positive emotions trigger upward spirals toward emotional well-being. Psychological Science, 13(2), 172–175.
https://doi.org/10.1111/1467-9280.00431
Holmes, E. A., Lang, T. J., & Shah, D. M. (2009). Developing interpretation bias modification as a “cognitive vaccine” for depressed mood: Imagining positive events makes you feel better than thinking about them verbally. Journal of Abnormal Psychology, 118(1), 76–88.
https://doi.org/10.1037/a0012590
Jaberghaderi, N., Greenwald, R., Rubin, A., Zand, S. O., & Dolatabadi, S. (2004). A comparison of CBT and EMDR for sexually-abused Iranian girls. Clinical Psychology & Psychotherapy: An International Journal of Theory & Practice, 11(5), 358–368.
https://doi.org/10.1002/cpp.395
Jiang, S. (2020). Don’t rush to deploy COVID-19 vaccines and drugs without sufficient safety guarantees. Nature, 579, Article 321.
https://doi.org/10.1038/d41586-020-00751-9
Kennard, B. D., Silva, S. G., Tonev, S., Rohde, P., Hughes, J. L., Vitiello, B., … March, J. (2009). Remission and recovery in the treatment for adolescents with depression study (TADS): Acute and long-term outcomes. Journal of the American Academy of Child & Adolescent Psychiatry, 48(2), 186–195.
https://doi.org/10.1097/CHI.0b013e31819176f9
Liu, N., Zhang, F., Wei, C., Jia, Y., Shang, Z., Sun, L., … Liu, W. (2020). Prevalence and predictors of PTSS during COVID-19 outbreak in China hardest-hit areas: Gender differences matter. Psychiatry Research, 287, Article 112921.
https://doi.org/10.1016/j.psychres.2020.112921
Mackinnon, A., Jorm, A. F., Christensen, H., Korten, A. E., Jacomb, P. A., & Rodgers, B. (1999). A short form of the Positive and Negative Affect Schedule: Evaluation of factorial validity and invariance across demographic variables in a community sample. Personality and Individual Differences, 27(3), 405–416.
https://doi.org/10.1016/S0191-8869(98)00251-7
Marrero, R. J., Carballeira, M., Martín, S., Mejías, M., & Hernández, J. A. (2016). Effectiveness of a positive psychology intervention combined with cognitive behavioral therapy in university students [In Spanish]. Anales de Psicología, 32(3), 728–740.
https://doi.org/10.6018/analesps.32.3.261661
Seligman, M. E. P. (2012). Flourish: A visionary new understanding of happiness and well-being. Simon & Schuster, Atria Books.
Seligman, M. E. P., & Csikszentmihalyi, M. (2000). Positive psychology: An introduction. American Psychologist, 55(1), 5–14.
https://doi.org/10.1037/0003-066X.55.1.5
Seligman, M. E. P., Rashid, T., & Parks, A. C. (2006). Positive psychotherapy. American Psychologist, 61(8), 774–788.
https://doi.org/10.1037/0003-066X.61.8.774
Sheldon, K. M., & Lyubomirsky, S. (2006). How to increase and sustain positive emotion: The effects of expressing gratitude and visualizing best possible selves. The Journal of Positive Psychology, 1(2), 73–82.
https://doi.org/10.1080/17439760500510676
Van Bortel, T., Basnayake, A., Wurie, F., Jambai, M., Koroma, A. S., Muana, A. T., … Nellums, L. B. (2016). Psychosocial effects of an Ebola outbreak at individual, community, and international levels. Bulletin of the World Health Organization, 94(3), 210–214. https://bit.ly/334LC0s
Walsh, S., Cassidy, M., & Priebe, S. (2016). The application of positive psychotherapy in mental health care: A systematic review. Journal of Clinical Psychology, 73(6), 638–651.
https://doi.org/10.1002/jclp.22368
Wang, C., & Zhao, H. (2020). The impact of COVID-19 on anxiety in Chinese university students. Frontiers in Psychology, 11, Article 01168.
https://doi.org/10.3389/fpsyg.2020.01168
Watson, D., Wiese, D., Vaidya, J., & Tellegen, A. (1999). The two general activation systems of affect: Structural findings, evolutionary considerations, and psychobiological evidence. Journal of Personality and Social Psychology, 76(5), 820–838.
https://doi.org/10.1037/0022-3514.76.5.820
World Health Organization. (n.d.). Coronavirus disease (COVID-19) pandemic. Author. https://bit.ly/2TO04Zk
Antoine, P., Dauvier, B., Andreotti, E., & Congard, A. (2018). Individual differences in the effects of a positive psychology intervention: Applied psychology. Personality and Individual Differences, 122, 140–147.
https://doi.org/10.1016/j.paid.2017.10.024
Bowen, M. (2020). COVID-19 has changed how we teach students. The Veterinary Record, 186(14), 461.
https://doi.org/10.1136/vr.m1535
Conoley, C. W., Pontrelli, M. E., Oromendia, M. F., Del Carmen Bello, B., & Nagata, C. M. (2015). Positive empathy: A therapeutic skill inspired by positive psychology. Journal of Clinical Psychology, 71(6), 575–583.
https://doi.org/10.1002/jclp.22175
Diener, E., Suh, E. M., Lucas, R. E., & Smith, H. L. (1999). Subjective well-being: Three decades of progress. Psychological Bulletin, 125(2), 276–302.
https://doi.org/10.1037/0033-2909.125.2.276
Fredrickson, B. L., & Joiner, T. (2002). Positive emotions trigger upward spirals toward emotional well-being. Psychological Science, 13(2), 172–175.
https://doi.org/10.1111/1467-9280.00431
Holmes, E. A., Lang, T. J., & Shah, D. M. (2009). Developing interpretation bias modification as a “cognitive vaccine” for depressed mood: Imagining positive events makes you feel better than thinking about them verbally. Journal of Abnormal Psychology, 118(1), 76–88.
https://doi.org/10.1037/a0012590
Jaberghaderi, N., Greenwald, R., Rubin, A., Zand, S. O., & Dolatabadi, S. (2004). A comparison of CBT and EMDR for sexually-abused Iranian girls. Clinical Psychology & Psychotherapy: An International Journal of Theory & Practice, 11(5), 358–368.
https://doi.org/10.1002/cpp.395
Jiang, S. (2020). Don’t rush to deploy COVID-19 vaccines and drugs without sufficient safety guarantees. Nature, 579, Article 321.
https://doi.org/10.1038/d41586-020-00751-9
Kennard, B. D., Silva, S. G., Tonev, S., Rohde, P., Hughes, J. L., Vitiello, B., … March, J. (2009). Remission and recovery in the treatment for adolescents with depression study (TADS): Acute and long-term outcomes. Journal of the American Academy of Child & Adolescent Psychiatry, 48(2), 186–195.
https://doi.org/10.1097/CHI.0b013e31819176f9
Liu, N., Zhang, F., Wei, C., Jia, Y., Shang, Z., Sun, L., … Liu, W. (2020). Prevalence and predictors of PTSS during COVID-19 outbreak in China hardest-hit areas: Gender differences matter. Psychiatry Research, 287, Article 112921.
https://doi.org/10.1016/j.psychres.2020.112921
Mackinnon, A., Jorm, A. F., Christensen, H., Korten, A. E., Jacomb, P. A., & Rodgers, B. (1999). A short form of the Positive and Negative Affect Schedule: Evaluation of factorial validity and invariance across demographic variables in a community sample. Personality and Individual Differences, 27(3), 405–416.
https://doi.org/10.1016/S0191-8869(98)00251-7
Marrero, R. J., Carballeira, M., Martín, S., Mejías, M., & Hernández, J. A. (2016). Effectiveness of a positive psychology intervention combined with cognitive behavioral therapy in university students [In Spanish]. Anales de Psicología, 32(3), 728–740.
https://doi.org/10.6018/analesps.32.3.261661
Seligman, M. E. P. (2012). Flourish: A visionary new understanding of happiness and well-being. Simon & Schuster, Atria Books.
Seligman, M. E. P., & Csikszentmihalyi, M. (2000). Positive psychology: An introduction. American Psychologist, 55(1), 5–14.
https://doi.org/10.1037/0003-066X.55.1.5
Seligman, M. E. P., Rashid, T., & Parks, A. C. (2006). Positive psychotherapy. American Psychologist, 61(8), 774–788.
https://doi.org/10.1037/0003-066X.61.8.774
Sheldon, K. M., & Lyubomirsky, S. (2006). How to increase and sustain positive emotion: The effects of expressing gratitude and visualizing best possible selves. The Journal of Positive Psychology, 1(2), 73–82.
https://doi.org/10.1080/17439760500510676
Van Bortel, T., Basnayake, A., Wurie, F., Jambai, M., Koroma, A. S., Muana, A. T., … Nellums, L. B. (2016). Psychosocial effects of an Ebola outbreak at individual, community, and international levels. Bulletin of the World Health Organization, 94(3), 210–214. https://bit.ly/334LC0s
Walsh, S., Cassidy, M., & Priebe, S. (2016). The application of positive psychotherapy in mental health care: A systematic review. Journal of Clinical Psychology, 73(6), 638–651.
https://doi.org/10.1002/jclp.22368
Wang, C., & Zhao, H. (2020). The impact of COVID-19 on anxiety in Chinese university students. Frontiers in Psychology, 11, Article 01168.
https://doi.org/10.3389/fpsyg.2020.01168
Watson, D., Wiese, D., Vaidya, J., & Tellegen, A. (1999). The two general activation systems of affect: Structural findings, evolutionary considerations, and psychobiological evidence. Journal of Personality and Social Psychology, 76(5), 820–838.
https://doi.org/10.1037/0022-3514.76.5.820
World Health Organization. (n.d.). Coronavirus disease (COVID-19) pandemic. Author. https://bit.ly/2TO04Zk
Figure 1. Experimental Timeline for Both Groups
Note. B1 = baseline measurement; TS = treatment sessions for PPI group; HR = health reminders for control group; Post = posttreatment assessment; 3-mon = follow-up assessment after 3 months; 6-mon = follow-up assessment after 6 months.
Table 1. Baseline Characteristics and Affective State of Participants
Note. PPI = positive psychology intervention; PA = positive affect score; NA = negative affect score.
Table 2. Summary of Interaction Effects and 95% Confidence Intervals for Positive Affect Scores According to Condition
Note. LL = lower limit; UL = upper limit.
Figure 2. Positive Affect Score in Both Groups
Note. PA = positive affect.
Figure 3. Negative Affect Score in Both Groups
Note. NA = negative affect.
Table 3. Means and Standard Deviations for the Main Effects of Positive and Negative Affect According to Condition
Note. PPI = positive psychology intervention.
Table 4. Summary of Interaction Effects and 95% Confidence Intervals for Negative Affect Score According to Condition
Note. LL = lower limit; UL = upper limit.
This paper was funded by the Heilongjiang Province Philosophy and Social Sciences Research Project (18KSB053).
Special thanks to Kaifeng Yin from Heilongjiang University of Science and Technology for providing dedicated help in academic instructions and language assistance.
Kunyan Liu, School of Computer Science and Technology, Harbin University of Science and Technology, No. 52 Xuefu Road, Nangang District, Harbin City, Heilongjiang Province, People’s Republic of China, 150080. Email: [email protected]